Prescription Psychiatric Medications
This module is a foil to everything before it. As technology advances, psychiatric medications become more specific, leading to more targeted benefits.
Note on structure: This module does not follow the Step 1→4 template used in Modules 4–7. Each drug class is covered by its mechanism, how the brain adapts, and the long-term side effects that result from that adaptation.
Modules 4–7 covered drugs built to be felt - large, rapid, unphysiological shifts in one system. Psychiatric medications are the opposite: slow, specific, subtle. They shift one system in one direction and wait for the brain to adapt. The adaptation is usually the treatment, not the drug's immediate action. This is why they take weeks to work and recreational drugs take minutes.
The side effects in this module are a different kind of side effect than the ones in Modules 4–7. A psychedelic's side effects are acute - they happen during the few hours the drug occupies its receptor, and they stop when the drug clears. Psychiatric drug side effects are mostly long-term: they come from a receptor being held in a non-baseline state constantly, for months or years. The brain responds to that constant pressure by remodelling - changing receptor numbers, sensitivity, downstream signalling. The side effect is the remodelling. This is why psychiatric side effects often appear after weeks on the drug, evolve over time, and sometimes persist after stopping - the opposite of the wears-off-by-morning psychedelic profile.
8.1 - SSRIs
Blocks SERT, the serotonin transporter that clears serotonin from the synapse. Slows cleanup of the brain's own signal.
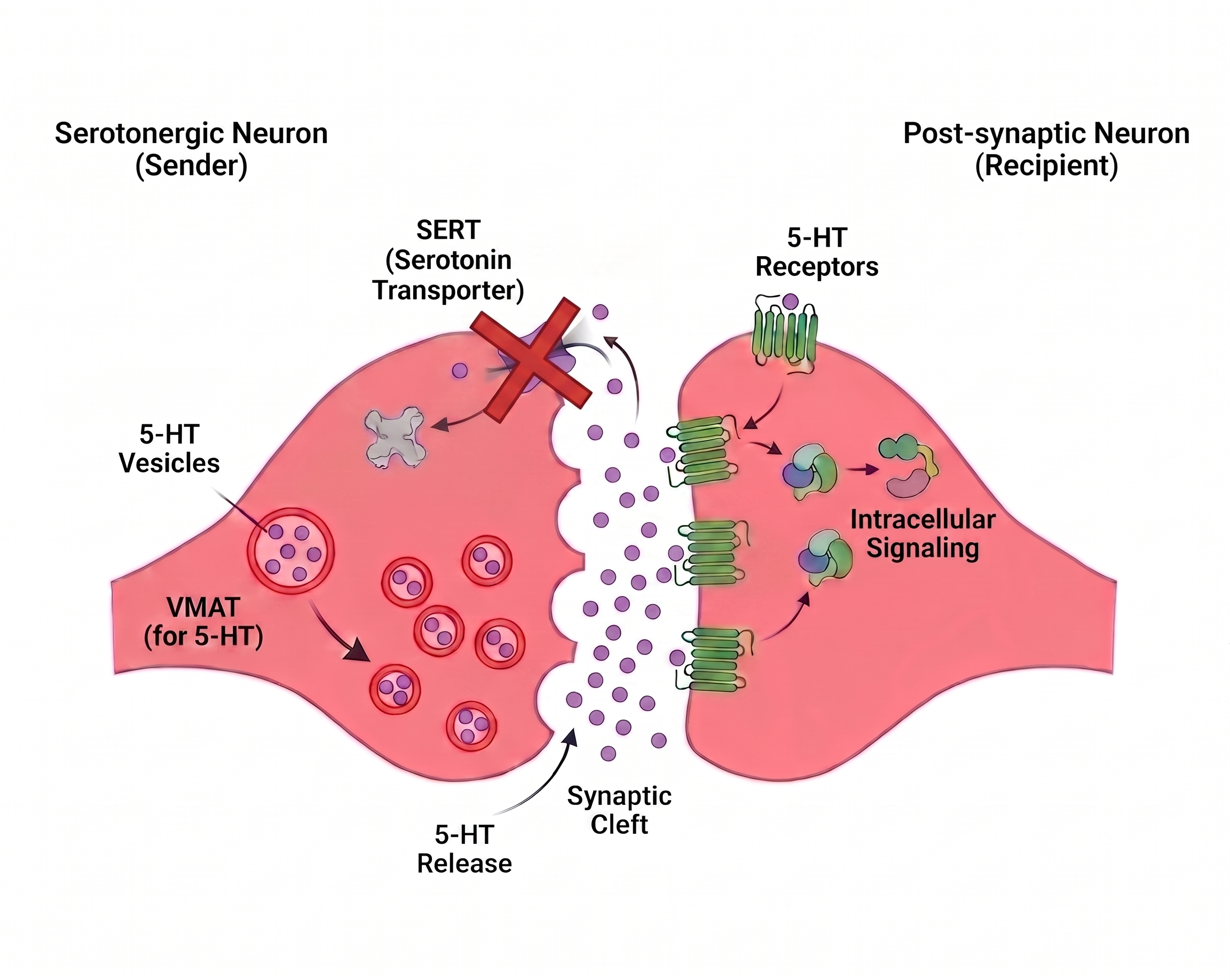
A key point on specificity: An SSRI acts at one transporter, but serotonin then drifts onto every serotonin receptor downstream. Serotonin landing on 5-HT1A is thought to carry the antidepressant benefit; serotonin landing on 5-HT2A and 5-HT2C causes most of the side effects. The "selective" in SSRI means selective for the transporter, not the receptors.
Serotonin rises within hours. But 5-HT1A autoreceptors on the serotonin neuron's own cell body sense the rise and brake the neuron's firing. More serotonin sitting there, fewer firing events sending it - roughly cancels out.
Those 5-HT1A autoreceptors desensitizing over 2–4 weeks. Now the neuron fires normally and reuptake is still blocked.
Sustained serotonin elevation; antidepressant effect emerges. The delay is the time the brake takes to wear out (Artigas et al., 2018; Albert et al., 2019).
Sexual dysfunction (lowered libido, delayed orgasm)
Constant 5-HT2A and 5-HT2C stimulation suppresses downstream dopamine signalling in pathways governing arousal. Unlike the early jitteriness, this often does not fade with adaptation; the receptor is being held stimulated indefinitely (Clayton et al., 2014).
Emotional blunting
Sustained 5-HT2A/2C tone dampens the dynamic range of emotional response. A months-long phenomenon, not an acute one; it builds as the brain settles into the new serotonergic set-point (Goodwin et al., 2017).
Discontinuation syndrome
The flip side of adaptation. After months, postsynaptic receptors have down-regulated to match the constant elevated serotonin. Stop suddenly → serotonin drops but the down-regulated receptors are still down-regulated → temporary signalling deficit ("brain zaps," dizziness, mood disturbance) until they re-adapt (Fava et al., 2015).
(Early effects such as nausea and jitteriness are the short-term exception here, and they mostly fade. The effects above are the long-term ones, and they behave differently because they're remodelling, not acute stimulation.)
8.2 - SNRIs
Blocks SERT and NET: serotonin reuptake like an SSRI, plus norepinephrine reuptake. Often dose-dependent: low doses act mostly like an SSRI; the norepinephrine effect kicks in higher.
The serotonin half follows the exact SSRI story - same 5-HT1A autoreceptor brake, same desensitization delay, same receptor split. The norepinephrine half raises noradrenergic tone.
Same delayed antidepressant effect as SSRIs, plus norepinephrine effects useful for chronic pain (descending pain pathways are noradrenergic).
Serotonergic long-term profile (shared with SSRIs)
Sexual dysfunction and emotional blunting via the same 5-HT2A/2C mechanism described in 8.1.
Sustained blood pressure elevation
Constant NET blockade means norepinephrine stays elevated at α- and β-adrenergic receptors on the vasculature and heart indefinitely → a chronic, low-grade pressor effect that builds over time and needs monitoring (Thase, 1998).
Worse discontinuation syndrome than most SSRIs
Especially venlafaxine; same remodelling logic, made sharper by a short half-life: the drug clears before the brain can re-adapt gradually.
8.3 - Mixed Opioid + SNRI
- Weak MOR agonism - the parent drug barely binds MOR, but its metabolite O-desmethyltramadol (M1) has ~200× higher affinity and produces most of the opioid effect (Grond & Sablotzki, 2004).
- Serotonin and norepinephrine reuptake inhibition - tramadol blocks SERT and NET like an SNRI antidepressant (Subedi et al., 2019).
- Serotonin syndrome when combined with SSRIs, SNRIs, MAOIs, or other serotonergic drugs.
- Lowered seizure threshold. Tramadol causes seizures at therapeutic doses, especially in overdose, via allosteric modulation of GABA-A benzodiazepine binding site (Lagard et al., 2022).
- Withdrawal includes both opioid withdrawal and SNRI-like discontinuation symptoms (brain zaps, anxiety, paresthesias).
You cannot reason about tramadol from Module 4 alone. Half its risks come from Module 8 machinery.
8.4 - Antipsychotics
Blocks D2 dopamine receptors. In psychosis, excess dopamine in the mesolimbic pathway drives hallucinations and delusions; blocking D2 there reduces that signalling. The opposite of stimulants, which raise dopamine.
D2 gets blocked in the target pathway, but D2 exists in other pathways too, and the drug can't tell them apart.
In pathways where D2 is blocked constantly, neurons build more D2 receptors to compensate for the chronic blockade.
Psychosis symptoms drop (the goal), but the off-target blockade and the compensation produce long-term side effects.
Acute movement effects (tremor, stiffness, restlessness)
From D2 blockade in the motor pathway. These are the relatively short-term effects - present while the drug is on board.
Tardive dyskinesia
The long-term one. Months to years of constant motor-pathway D2 blockade drive that pathway to up-regulate D2 receptors; eventually the over-supplied pathway produces involuntary movements (lip-smacking, facial movements) that may persist after the drug is stopped (Waln & Jankovic, 2013). This is the clearest example in the module of a long-term side effect being the remodelling itself, following the same receptor-upregulation logic as the withdrawal sections earlier in the course.
Hyperprolactinemia
D2 normally suppresses prolactin release; block it constantly → prolactin stays chronically elevated → menstrual disruption, breast changes, lowered bone density over time (Peuskens et al., 2014).
Metabolic syndrome (weight gain, insulin resistance, especially olanzapine)
A slow, cumulative effect of sustained action at H1 and 5-HT2C receptors involved in appetite and metabolism, building over months on the drug (Reynolds & Kirk, 2010).
Note: still no "high" - antipsychotics are corrective, not euphoric.
8.5 - Mood Stabilizers
The most diffuse drugs here. Instead of grabbing one receptor, they work upstream on the polarization of neurons, the ion-channel machinery from Module 1. Lamotrigine and valproate block voltage-gated sodium channels (less influx → harder to push neurons to threshold); valproate also raises GABA; lithium acts on intracellular signalling enzymes.
Neurons become less prone to extreme firing in either direction - the peaks and troughs of mood flatten. A well-controlled person doesn't feel "on a drug"; the swings just get smaller.
Because these act on ion channels and signalling cascades found body-wide, their long-term effects are about cumulative organ exposure rather than receptor remodelling.
Lithium - thyroid and kidney damage
Lithium has a narrow therapeutic index and, over years, can cause thyroid and kidney damage, a slow toxicity that requires ongoing blood monitoring (McKnight et al., 2012). The mechanism story here is less "receptor adapts" and more "a body-wide target stressed continuously."
Valproate - liver and metabolic burden
Long-term liver enzyme elevation and weight gain. Also carries teratogenicity risk requiring monitoring in people of childbearing potential.
Lamotrigine - Stevens-Johnson rash risk during titration
The best-tolerated mood stabilizer for most people, but the dose must be built slowly because rapid titration raises the risk of Stevens-Johnson syndrome (a rare, serious rash). The payoff: once at dose, it's generally well tolerated long-term.
Lamotrigine is the most well tolerated but takes the longest to build to a therapeutic dose - watch out for the rash though.
8.6 - MAOIs
MAOIs are older psychiatric medications, largely replaced in mainstream use by SSRIs.
MAOIs block monoamine oxidase (the enzyme that breaks down all the monoamines), so serotonin, norepinephrine, and dopamine all build up at once.
Effective, but the least specific drug in the module - which is exactly why it fell out of use. The arc of psychiatric pharmacology is the move away from broad drugs like this toward narrow ones like SSRIs (Finberg & Rabey, 2016).
User Manual
Focusing on a narrow target is typically how psychiatric medications work. As technology advances and we can more effectively do this, the long-term efficacy gets better as well as usefulness. Side-effect profiles decrease; benefits we want increase.
Their adaptation is exactly where their side effects come from - a receptor held in a non-baseline state for months or years, and the brain remodelling around it. That's why psychiatric side effects appear late, evolve slowly, and can outlast the drug. They're not the drug acting; they're the brain adapting.
Because the brain adapts around these drugs, they can't be stopped abruptly. The remodelling is still in place when the drug is gone, which is what causes discontinuation effects. Always taper under medical supervision.
SSRIs and antipsychotics produce discontinuation effects; stopping abruptly is uncomfortable but not life-threatening. However, some psychiatric medications are GABAergic (benzodiazepines, barbiturates, GHB) - stopping those abruptly can cause seizures and death. See Module 6: Depressants for the mechanism and why the GABAergic class is categorically different.
Sources
- Albert, P. R., et al. (2019). Serotonin-1A autoreceptors and depression: from genes to receptors to behavior. Trends in Neurosciences, 42(3), 172–186. https://doi.org/10.1016/j.tins.2018.10.003
- Artigas, F., et al. (2018). Serotonin and antidepressants: new views from microdialysis studies. Trends in Pharmacological Sciences, 39(3), 262–273. https://doi.org/10.1016/j.tips.2017.12.004
- Clayton, A. H., et al. (2014). Antidepressant-associated sexual dysfunction: a potentially avoidable therapeutic challenge. Postgraduate Medicine, 126(2), 91–99. https://doi.org/10.3810/pgm.2014.03.2744
- Fava, G. A., et al. (2015). Withdrawal symptoms after selective serotonin reuptake inhibitor discontinuation: a systematic review. Psychotherapy and Psychosomatics, 84(2), 72–81. https://doi.org/10.1159/000370338
- Finberg, J. P. M., & Rabey, J. M. (2016). Inhibitors of MAO-A and MAO-B in psychiatry and neurology. Frontiers in Pharmacology, 7, 340. https://doi.org/10.3389/fphar.2016.00340
- Goodwin, G. M., et al. (2017). Emotional blunting with antidepressant treatments: a survey among depressed patients. Journal of Affective Disorders, 221, 31–35. https://doi.org/10.1016/j.jad.2017.05.048
- Grond, S., & Sablotzki, A. (2004). Clinical pharmacology of tramadol. Clinical Pharmacokinetics, 43(13), 879–923. https://doi.org/10.2165/00003088-200443130-00004
- Lagard, C., et al. (2022). Investigation of the mechanisms of tramadol-induced seizures in overdose in the rat. Pharmaceuticals, 15(10), 1254. https://doi.org/10.3390/ph15101254
- McKnight, R. F., et al. (2012). Lithium toxicity profile: a systematic review and meta-analysis. The Lancet, 379(9817), 721–728. https://doi.org/10.1016/S0140-6736(11)61516-X
- Peuskens, J., et al. (2014). The effects of novel and newly approved antipsychotics on serum prolactin levels: a comprehensive review. CNS Drugs, 28(5), 421–453. https://doi.org/10.1007/s40263-014-0157-3
- Reynolds, G. P., & Kirk, S. L. (2010). Metabolic side effects of antipsychotic drug treatment - pharmacological mechanisms. Pharmacology & Therapeutics, 125(1), 169–179. https://doi.org/10.1016/j.pharmthera.2009.10.010
- Subedi, M., et al. (2019). Tramadol: understanding the risk of serotonin syndrome and seizures. American Journal of Medicine, 132(2), 161–168. https://doi.org/10.1016/j.amjmed.2018.09.017
- Thase, M. E. (1998). Effects of venlafaxine on blood pressure: a meta-analysis of original data from 3744 depressed patients. Journal of Clinical Psychiatry, 59(10), 502–508. https://doi.org/10.4088/jcp.v59n1002
- Waln, O., & Jankovic, J. (2013). An update on tardive dyskinesia: from phenomenology to treatment. Tremor and Other Hyperkinetic Movements, 3, tre-03-161-4138-1. https://doi.org/10.7916/D88P5Z71