Cannabinoids
Natural cannabis carries real but manageable risks at moderate use. Synthetic cannabinoids ("K2," "Spice") are categorically different; full CB1 agonism produces a toxicity profile that includes seizures, psychosis, and acute kidney injury, and they should not be treated as a cannabis substitute.
Also cannabis has a lot LOT more going on when it comes to terpenes and the entourage effect - more on that in Submodule 10a.2: Cannabis vs. Isolated THC.
Step 1: What the Drug Does
THC is a partial agonist at CB1 receptors. It enters from outside and activates CB1 receptors broadly. CB1 activation inhibits voltage-gated Ca²⁺ channels and opens K⁺ channels:
presynaptic terminal hyperpolarized → less neurotransmitter released from that terminal
Synthetic cannabinoids ("K2," "Spice") are full agonists with much higher potency. They produce far more severe acute toxicity than natural cannabis: seizures, psychosis, and acute kidney injury rarely seen with cannabis (Tai & Fantegrossi, 2014).
One-line summary: THC = "reduces presynaptic neurotransmitter release at every neuron that has a CB1 receptor (GABA, glutamate, and others)."
Step 2: What the Endocannabinoid System Normally Does
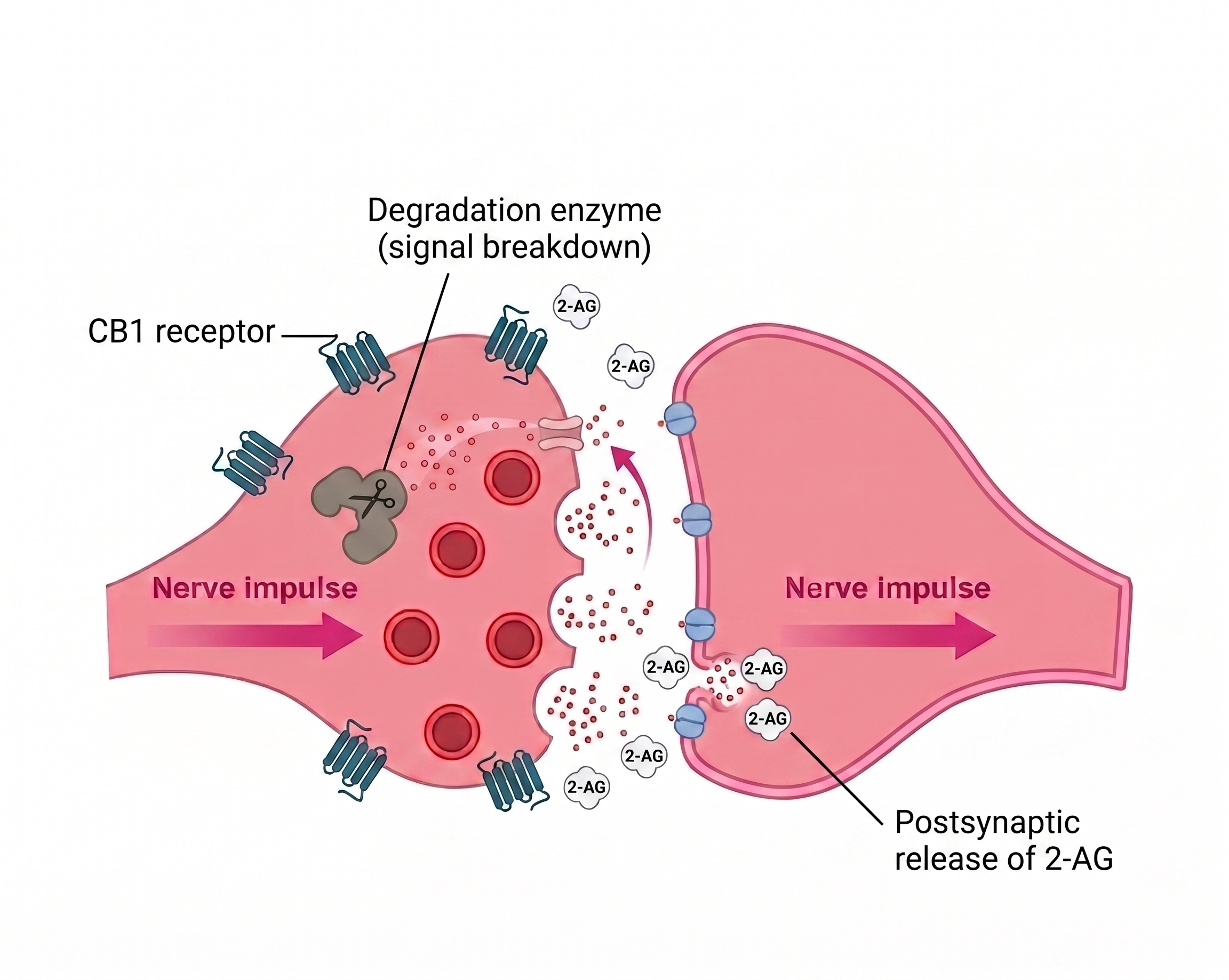
The endocannabinoid system is retrograde: the postsynaptic (receiving) neuron makes endocannabinoids on demand and sends them backwards across the synapse. They bind CB1 on the presynaptic terminal and inhibit further neurotransmitter release from that terminal.
The receiver signals the sender to reduce output, a feedback control mechanism activated selectively when the receiving neuron has excess input (Lu & Mackie, 2016). The typical endocannabinoid for this is 2-AG, as shown in the image above. The system operates on glutamate, GABA, and other synapse types.
THC is different: it activates CB1 receptors from outside, reaching every CB1 receptor regardless of whether any receiving neuron signaled for it. In the case of full agonists like K2 or Spice, CB1 is fully activated - producing the overdose picture.
Step 3: Where CB1 Lives

 img.png)
Step 4: How Side Effects Fall Out of Steps 1–3
Euphoria
VTA CB1 receptors sit on GABAergic interneuron terminals. Activation suppresses GABA release → dopamine neurons are disinhibited → dopamine flows into NAc. Same disinhibition logic as opioids and benzos; different receptor, same downstream result.
↑
Short-Term Memory Impairment
Hippocampal CB1 activation suppresses glutamate release → no LTP → no new memories formed while intoxicated. This is a direct pharmacological effect, not cognitive style; the cellular machinery for memory encoding is turned off.
↓
Motor Coordination Problems
Cerebellar and basal ganglia CB1 activation suppresses motor signaling → ataxia, slowed reflexes, impaired fine motor control. Driving under cannabis impairment is measurably dangerous, even when users feel unimpaired.
↓
Anxiety / Paranoia at High Doses
Amygdala CB1 has biphasic effects: anxiolytic at low doses, anxiogenic at high doses (a U-shaped curve). The reason isn't fully understood; it likely involves different CB1 populations on excitatory vs. inhibitory neurons shifting their relative balance as doses escalate.
↑
Acute Psychosis (Rare with Cannabis, More Common with Synthetics)
Mechanism not fully understood. Likely involves disrupted balance between cortical excitation and inhibition; also strain-dependent; THC:CBD ratio matters (CBD partially counteracts THC's psychotogenic effects).
Cannabis Hyperemesis Syndrome
Chronic heavy use produces paradoxical, severe cyclical vomiting (paradoxical because acute cannabis is antiemetic). Mechanism still being characterized; likely involves CB1 dysregulation in the gut and brainstem nausea centers. The classic tell: relief from hot showers (capsaicin-adjacent thermoreceptor mechanism).
The Balancing Loop
Chronic CB1 activation → β-arrestin recruitment → CB1 internalization → receptor downregulation (Oviedo et al., 1993). Tolerance builds. Withdrawal is real but mild compared to opioids or benzos:
- Irritability
- Sleep disturbance
- Decreased appetite
- Mood disturbance
- Peak intensity at days 2–6 after cessation

User Manual
Most-cited risks (memory, psychosis vulnerability, dependence) scale with potency, frequency of use, and age of first use. Adolescent cannabis use is associated with measurable changes in cortical maturation (Volkow et al., 2014). The risks from natural cannabis are real but manageable; the risks from synthetic cannabinoids are categorically different.
Synthetic cannabinoids ("K2," "Spice") deserve a separate warning. Full-agonist activity at CB1 can produce seizures, severe psychosis, and acute kidney injury rarely seen with cannabis. Higher-potency cannabis products (concentrates, dabs) push closer to this risk profile. Daily adolescent use is the strongest known risk factor for dependence and possibly persistent cognitive effects.
Sources
- Lu, H. C., & Mackie, K. (2016). An introduction to the endogenous cannabinoid system. Biological Psychiatry, 79(7), 516–525. https://doi.org/10.1016/j.biopsych.2015.07.028
- Oviedo, A., Glowa, J., & Herkenham, M. (1993). Chronic cannabinoid administration alters cannabinoid receptor binding in rat brain: a quantitative autoradiographic study. Brain Research, 616(1–2), 293–302. https://doi.org/10.1016/0006-8993(93)90222-L
- Tai, S., & Fantegrossi, W. E. (2014). Synthetic cannabinoids: pharmacology, behavioral effects, and abuse potential. Current Addiction Reports, 1(4), 239–246. https://doi.org/10.1007/s40429-014-0033-8
- Volkow, N. D., et al. (2014). Adverse health effects of marijuana use. New England Journal of Medicine, 370(23), 2219–2227. https://doi.org/10.1056/NEJMra1402309