Drug Interactions
Probably the most important module for harm reduction.
Most Drug Deaths Are Not Single-Drug Deaths
The numbers, from clinical and forensic data:
 Average number of drugs present per drug-involved death by year..png)
A single drug is comparatively predictable. You can reason about its receptor, its region, its dose. A combination is where the math stops being additive and people die at doses that, taken alone, each drug's user would have survived.
The Framework: Mechanism Stacking
Two drugs in the same body interact in one of three ways. Each is a direct extension of the receptor-and-region logic from earlier modules.
e.g., alcohol + benzo: same GABA-A brake, pressed twice.
How to use the framework: Take each drug, pull its mechanism from the relevant module, and check where the two mechanisms land. If they end at the same dangerous downstream effect, the combination is more dangerous than either part.
Example 1: Opioid + Benzodiazepine - Parallel Suppression
Pull the mechanisms from earlier modules.
- Opioid (Module 4): binds MOR on the preBötzinger Complex → silences the brainstem neurons that generate breathing rhythm → respiratory depression ↓
- Benzodiazepine (Module 6): positive allosteric modulator at GABA-A → amplifies chloride influx → hyperpolarizes neurons, including those in brainstem respiratory centers → respiratory depression ↓
Both end at the same place: breathing suppressed. They get there through different doors: one through MOR, one through GABA-A.
brainstem rhythm generator
in brainstem centers
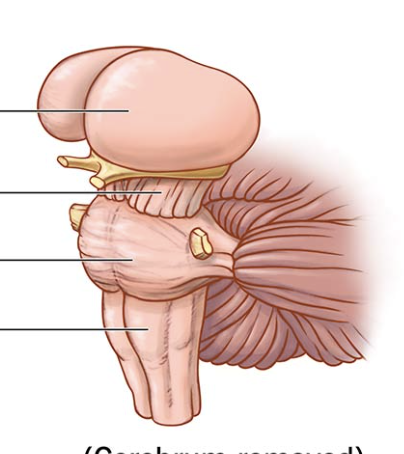
breathing ↓ ↓
Why the "benzo ceiling" doesn't help
Benzodiazepines have a built-in ceiling on their own: they only amplify existing GABA signaling, so pure benzo overdose rarely kills. But that ceiling is built around the GABA-A mechanism. It does nothing to limit the opioid's MOR-driven suppression. The two mechanisms suppress breathing in parallel, and neither one's safety limit applies to the other.
Conclusion: the combination depresses breathing far more than either alone, and is fatal at doses each drug's user would individually survive. Opioids were present in roughly 85% of benzodiazepine-involved overdose deaths in one large dataset (Tori et al., 2020).
Now apply it to the current supply
Module 10 covers that most street "heroin" is fentanyl, and that fentanyl shows up as an undisclosed adulterant in other drugs. So a person taking a benzodiazepine (bought as a benzo, believed to be a benzo) that has been pressed or cut with fentanyl is unknowingly running the opioid + benzo parallel suppression in their own brainstem. Two independent mechanisms cutting breathing, no shared ceiling, and the person doesn't know one of the two drugs is even present. The framework predicts the outcome before any data is consulted.
Gustav Åhr (Lil Peep), 1996–2017. Died of a fentanyl-xanax combination in Tucson, Arizona, at 21 years old. The respiratory depression mechanism described above is the primary danger of this specific drug combination.
Example 2: Stimulant + Depressant - Mutual Masking
Common forms: cocaine + heroin, methamphetamine + opioid, cocaine + benzo.
Pull the mechanisms.
- Stimulant (Module 5): blocks DAT and NET → dopamine and norepinephrine accumulate in synapses. NE on α1 vessels → vasoconstriction, blood pressure up. NE on β1 heart → tachycardia. Cortical activation → user feels alert and awake.
- Opioid (Module 4): binds MOR → sedation, and suppression of the preBötC breathing rhythm.
Check where they land:
Two failure modes follow directly
Asymmetric clearance. Cocaine's half-life is ~30–90 minutes; heroin's active metabolites last ~4–6 hours. The stimulant clears first. The opioid respiratory depression keeps going - now without the cortical wake-up masking it. The person felt fine minutes ago and stops breathing.
Cardiovascular stress. Heart working hard against vasoconstricted vessels while the opioid depresses breathing and lowers oxygen. The result can be myocardial infarction or arrhythmia even when the respiratory depression alone would not have been fatal.
The epidemiology matches the prediction: combined stimulant-opioid use carries roughly 3–4× the fatal overdose rate of either drug used alone (Leri et al., 2003).
What the Framework Does Not Give You
Mechanism reasoning tells you whether two drugs collide and where. It does not give you thresholds. You cannot calculate a fatal dose from mechanism alone. The variables it leaves open:
- Route of administration
- Individual CYP450 enzymes that set how fast each drug is metabolized
- Current tolerance to each drug
- Body composition
- What is actually in the product (per Module 10)
The framework narrows the unknown. It does not eliminate it.
User Manual
Most overdose deaths are interaction deaths (Compton et al., 2021). The framework is the tool: for any combination, pull each drug's mechanism from its module, find where the mechanisms land, and check whether they stack, collide, or mask.
- If two drugs end at the same dangerous downstream effect (breathing, blood pressure, body temperature, serotonin load), that is parallel suppression or synergy, and the combination is more dangerous than the parts.
- Any combination involving a depressant (opioid, benzo, alcohol, GHB, gabapentinoid) deserves the most caution. The majority of polysubstance overdose deaths involve at least one.
- Because the current supply is contaminated (Module 10), every combination should be treated as potentially also containing fentanyl. A benzo cut with fentanyl is the opioid + benzo interaction whether or not the user intended it.
- "I feel okay" is not "I am okay." Mutual masking means the body can be failing while the user feels balanced. It is the leading reason people redose into a fatal stack.
- Harm-reduction interaction checkers (TripSit, Drugs.com) exist. Most fatal interactions are predictable before they happen.
Sources
- Centers for Disease Control and Prevention. (2024). Polysubstance overdose. CDC Overdose Prevention. https://www.cdc.gov/overdose-prevention/about/polysubstance-overdose.html
- Compton, W. M., Valentino, R. J., & DuPont, R. L. (2021). Polysubstance use in the U.S. opioid crisis. Molecular Psychiatry, 26(1), 41–50. https://doi.org/10.1038/s41380-020-00949-3
- Friedman, J. R., Romero, R., Funnell, A., Goodman-Meza, D., & Shover, C. L. (2026). What does 'polysubstance' really mean? Comparing drug-involved deaths in CDC records vs. detailed medical examiner data from Los Angeles. International Journal of Drug Policy, 148, 105129. https://doi.org/10.1016/j.drugpo.2025.105129 (data covers 2012–2023)
- Leri, F., Bruneau, J., & Stewart, J. (2003). Understanding polydrug use: review of heroin and cocaine co-use. Addiction, 98(1), 7–22. https://doi.org/10.1046/j.1360-0443.2003.00236.x
- Lippold, K. M., et al. (2021). Trends in unintentional polysubstance overdose deaths and individual and community correlates of polysubstance overdose, North Carolina, 2009–2018. Drug and Alcohol Dependence, 219, 108460. https://doi.org/10.1016/j.drugalcdep.2020.108460
- Tori, M. E., Larochelle, M. R., & Naimi, T. S. (2020). Alcohol or benzodiazepine co-involvement with opioid overdose deaths in the United States, 1999–2017. JAMA Network Open, 3(4), e202361. https://doi.org/10.1001/jamanetworkopen.2020.2361