Classic Psychedelics
This is the longest module.
Step 1: What the Drug Does
Classic psychedelics are serotonin receptor agonists. The differences in experience between psychedelics come from which serotonin receptors each drug binds, how strongly, and which intracellular signaling pathway gets triggered.
The serotonin system has at least 14 receptor subtypes. Four cover most of what you need to understand most psychedelics (three drive the psychological experience, one drives physiological risk), plus one more relevant to microdosing.
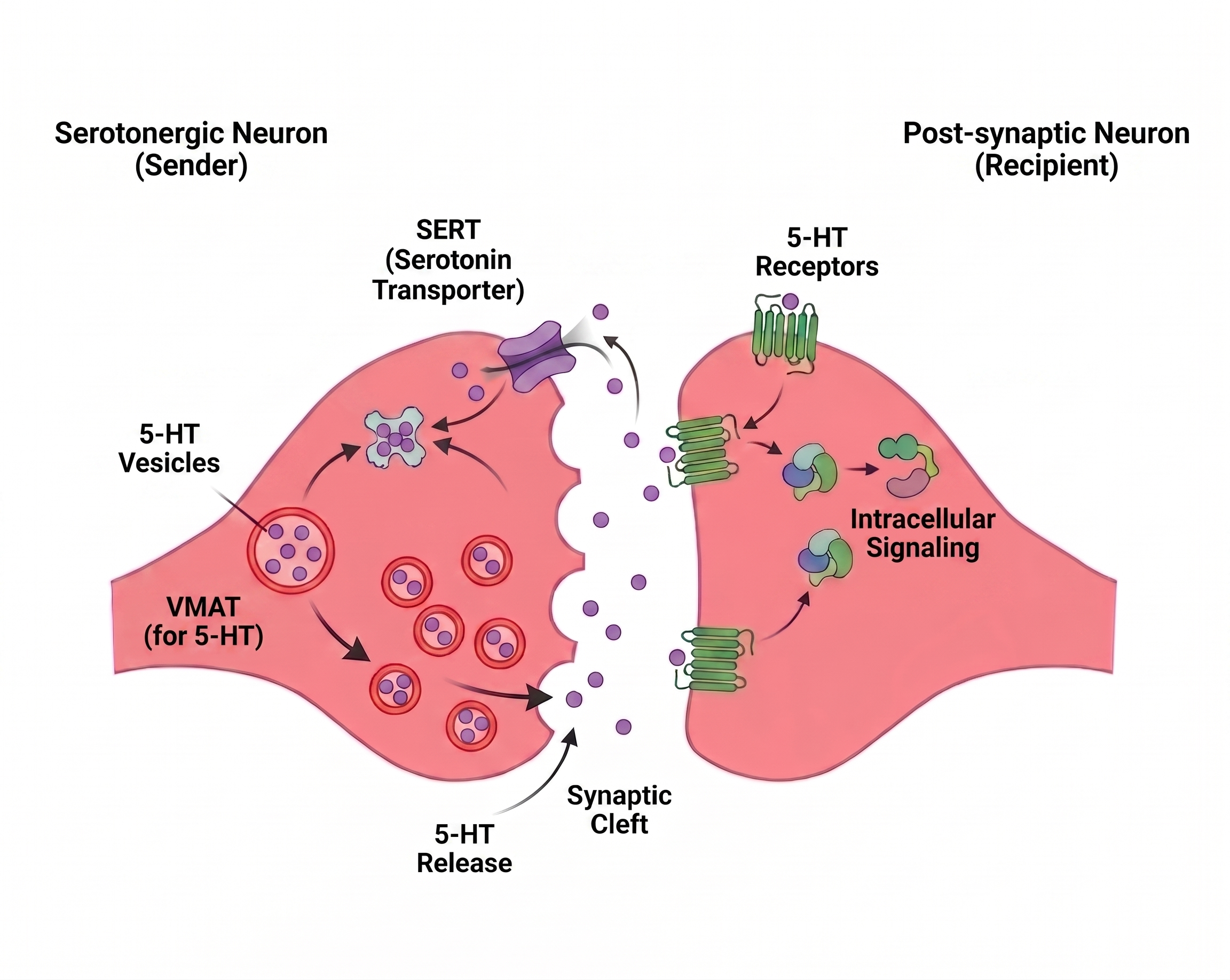
Video: Serotonin Synapse (in depth) - click to expand ↗ YouTube
hypothalamus & periphery
.png)
cardiac valves

The framework: different psychedelics produce different experiences and different risk profiles because they hit these five receptors in different ratios and signal through different downstream pathways.
Step 2: What These Serotonin Receptors Normally Do
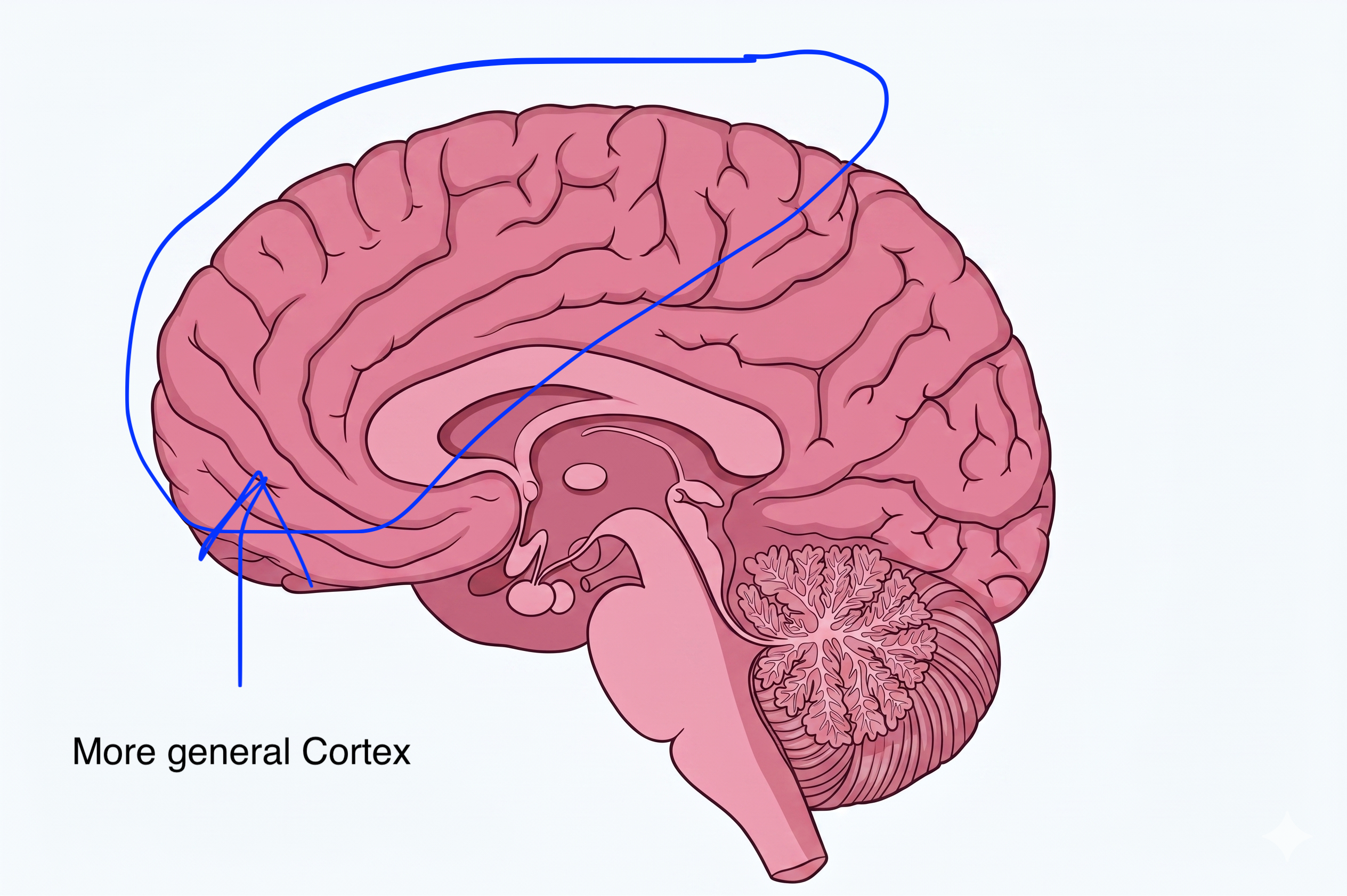
- 5-HT2A (cortex) acts as a sensitivity dial on cortical pyramidal neurons. Normal signaling helps the cortex respond appropriately to incoming sensory data while filtering out internally-generated noise. Override the dial → hallucinations.
- 5-HT2A (hypothalamus & periphery) normally helps fine-tune body temperature in response to serotonin signaling and contributes to baseline sympathetic tone. Overactivate it → thermoregulation goes off, sympathetic output spikes.
- 5-HT1A is the brain's "calm down" signal in the serotonin system. As an autoreceptor, it tells serotonin neurons to stop firing when serotonin levels rise. As a postsynaptic receptor, it directly hyperpolarizes target neurons.
- 5-HT2C modulates dopamine neuron firing. Affects mood, anxiety, and the emotional valence of an experience.
Step 3: Where These Receptors Live
Simplified to regions covered in this course. Each region's normal job is what gets altered when psychedelics activate its receptors.
↑ ↓
↓ img.png) ↑
↑ ↑↑↓↑
↑↑↓↑ ↑
↑Step 4: How 5-HT2A Agonism Typically Works
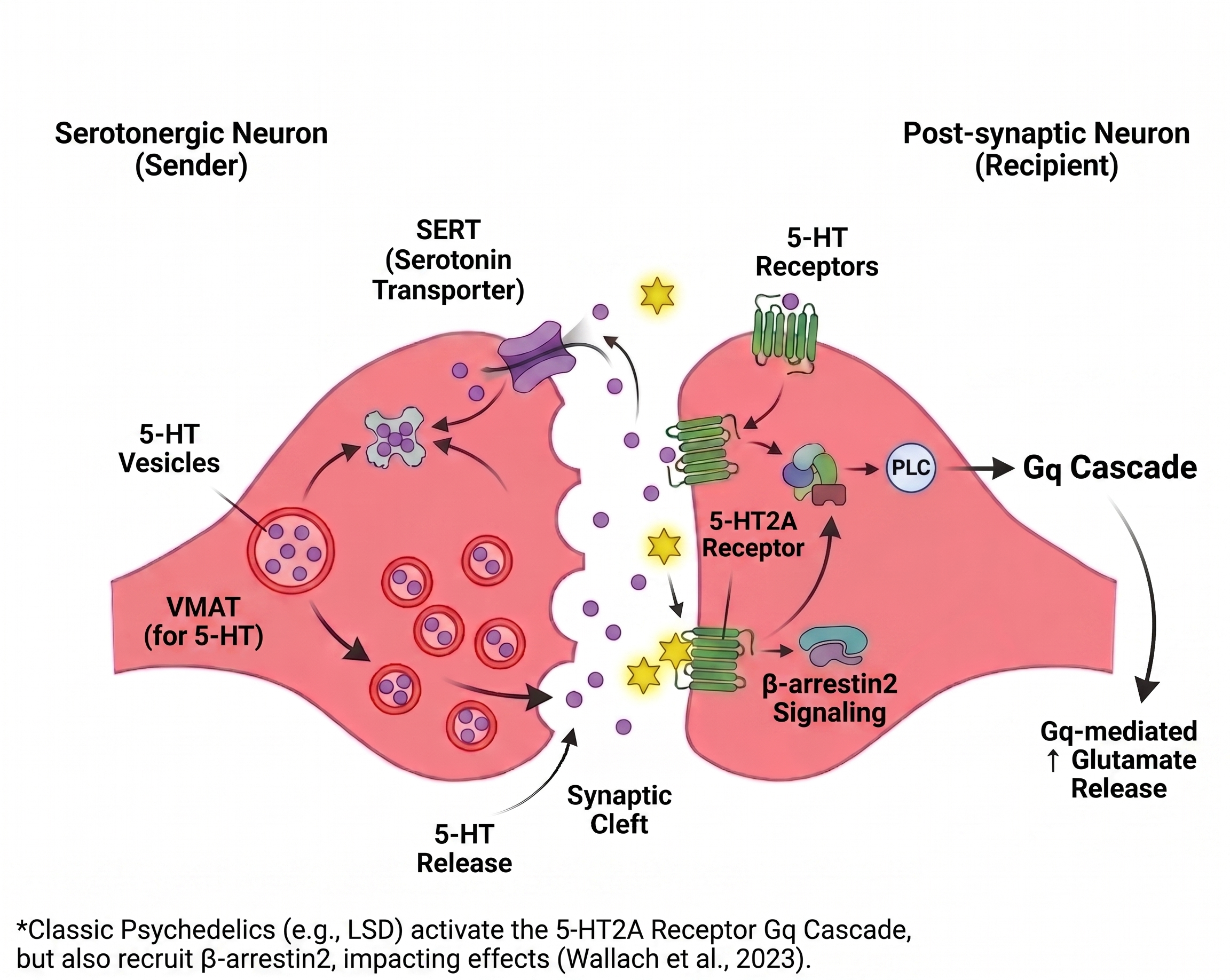
Classic psychedelics act as agonists at the serotonin 2A receptor (5-HT2A), a G-protein-coupled receptor densely expressed on layer V pyramidal neurons in the cortex.
Binding triggers a Gq cascade (via phospholipase C) → increases excitatory glutamate release in the cortex. Cortical pyramidal neurons receive persistent depolarizing input.
Glutamate release increases in the cortex. Neurons fire in patterns they normally would not generate.
 ↑
↑
Extra note: Psychedelics also recruit β-arrestin2 signaling at the same receptor. The balance between the Gq and β-arrestin pathways explains why some 5-HT2A agonists are not psychedelic - they preferentially activate one pathway over the other (Wallach et al., 2023). This is called biased agonism and is currently a major target in drug development.

One-line summary: Psychedelics = "force cortical pyramidal neurons to fire more, all at once."
Step 5: The 5-HT2A / 5-HT1A Ratio
The visual character of a psychedelic experience is determined by the ratio of 5-HT2A activation (excitation) to 5-HT1A activation (inhibition) in the cortex.
- Strong 5-HT2A + weak 5-HT1A → cortical hyperexcitation dominates → glutamate release increases in the visual cortex → strong visual hallucinations, "the world is changing."
- Strong 5-HT2A + strong 5-HT1A → 5-HT1A inhibition muffles the cortical hyperexcitation → minimal visuals despite 5-HT2A being engaged → profound DMN shutdown → "the self is dissolving" without "the world is changing."
This tug-of-war is pharmacologically verifiable. If 5-HT1A is selectively blocked, drugs that normally produce ego-death-without-visuals shift toward producing classical visual hallucinations (Halberstadt & Geyer, 2011). The 5-HT2A signal was always there - it was being overridden by 5-HT1A inhibition.
This is why 5-MeO-DMT (very high 5-HT1A relative to 5-HT2A) produces near-total ego dissolution with relatively few visuals, while LSD (high 5-HT2A relative to 5-HT1A) tends to produce vivid visual effects alongside ego disruption.
Step 6: Dose-Response - Why Higher Doses Are Categorically Different
The dose-response curve is non-linear. Below certain thresholds, effects like ego dissolution simply don't occur. Ranges from sub-perceptual microdoses (<15% receptor occupancy) to full ego dissolution at 60–70%+. Click to see the full dose table.
›
A psychedelic dose-response curve is not linear. Doubling the dose does not double the effect; the experience moves through distinct phases as more 5-HT2A receptors get occupied. Below specific thresholds, certain effects do not appear at all, no matter how long the user waits.
The mechanism is receptor occupancy. A standard 25 mg psilocybin dose occupies an estimated 60–70% of cortical 5-HT2A receptors (Madsen et al., 2019). A 5 mg "microdose" occupies far less - likely under 20%. Different brain regions also have different 5-HT2A receptor densities, so the same systemic occupancy translates to different functional effects in different regions.
1–3 mg
3–7 mg
7–15 mg
15–24 mg
25 mg+
- Not enough 5-HT2A receptors are occupied to drive the cortical glutamate increase needed to disrupt DMN connectivity.
- The DMN is robust - it takes substantial cortical disruption to break its synchronization. Partial 5-HT2A activation gets damped out by the rest of the network.
- Visual cortex has very dense 5-HT2A. Visual effects appear at lower doses than ego dissolution because V1 reaches its activation threshold sooner than DMN nodes do.
- The amygdala is dose-sensitive. Low doses produce mild emotional shifts; high doses can produce intense emotion in either direction.
Step 7: What a Trip Actually Looks Like - The Phenomenology
Onset (30–60 min) → come-up → peak (90 min–3 hr, potential ego dissolution) → plateau → comedown → afterglow over 1–3 days. The duration is governed by pharmacokinetics: DMT compresses the arc to ~15 min; LSD stretches it to 8–12 hr. Click to see the full timeline.
›
The receptor mechanism translates into a predictable arc. A typical moderate-to-high dose oral psilocybin trip:
-
Onset
30–60 min 5-HT2A receptors begin binding. Mild body load, sometimes nausea (5-HT3 activation in the gut). Increasing sense of anticipation or anxiety. Visual cortex starts showing very subtle pattern noise. -
Come-up
60–90 min Visuals build. Open-eye distortions: surfaces seem to "breathe," colors saturate, edges shimmer. Emotional sensitivity increases sharply. Music becomes vivid. Time perception begins to stretch. -
Peak
90 min–3 hr Maximum receptor occupancy. Closed-eye visuals can become geometric, fractal, or representational. Emotional content surfaces strongly - often including material the user wasn't conscious of beforehand. If the dose is high enough, ego dissolution onset here: the sense of "I" becomes thin, then dissolves. Distinction between self and surroundings blurs. Insights arrive with strong conviction. -
Plateau
3–5 hr Sustained high state. Cognitive flexibility extreme. Time sense unreliable. Body feels distant. -
Comedown
5–7 hr 5-HT2A occupancy drops. Visuals recede first. Sense of self gradually reassembles. Reflective phase - users often spend hours processing what they experienced. Mild physical fatigue. -
Afterglow
1–3 days Mood often elevated. Sense of openness, gratitude, or emotional clarity. Underlying mechanism: acute neuroplasticity (see Step 9).
The whole arc is governed by pharmacokinetics. Smoked DMT compresses the same arc into ~15 minutes because the drug reaches and clears 5-HT2A receptors rapidly. LSD stretches it to 8–12 hours because the molecule physically locks into the receptor for far longer than psilocin does - a "lid" formed by the receptor over the bound LSD molecule (Wacker et al., 2017).
Step 8: Bad Trips - The Amygdala Feedback Loop
A "bad trip" is not random. It has a specific mechanism: the amygdala gets amplified by 5-HT2A activation, and a feedback loop forms between fear, physical symptoms, and the user's interpretation of those symptoms.
The amygdala under psychedelics has heightened reactivity to emotionally significant stimuli (Kraehenmann et al., 2015). Whatever emotional state the user arrives with gets amplified by the same 5-HT2A activation producing the visuals. If the starting state is calm and trusting, the amplified emotion is positive. If the starting state is anxious or threatened, the amplified emotion is fear.

This loop has no built-in termination. Once running, it can sustain itself for hours, scaling with the duration of the drug's action.
What breaks the loop:
- Reduced sensory input. Dark, quiet room with a trusted person. Less raw input = less material for the amygdala to amplify.
- Cognitive reframing. "This is the drug. It will end. I am safe." The PFC can still partially override the amygdala if the loop hasn't progressed too far.
- Physical grounding. Holding ice, walking, touching textured objects - engaging the parasympathetic system to counter the sympathetic surge.
- Pharmacological interruption. Benzodiazepines (GABA-A potentiation overrides cortical hyperexcitation) or antipsychotics (D2/5-HT2A antagonism) shut down the trip in minutes if administered.
Set and setting are clinical requirements - they are direct inputs into the amygdala feedback loop, not just preferences.
Step 9: Acute Neuroplasticity - Why the Effects Outlast the Trip
Psychedelics acutely promote synaptic plasticity in the cortex. This happens through the same 5-HT2A activation but operates on a different timescale.
The mechanism (Ly et al., 2018; Vargas et al., 2023):
- 5-HT2A activation on cortical pyramidal neurons triggers Gq signaling and downstream pathways.
- This induces release of BDNF (brain-derived neurotrophic factor).
- BDNF activates TrkB receptors on the neuron.
- TrkB signaling promotes dendritic spine growth.
- This effect peaks 24–72 hours after a single dose and persists for at least 1 month in animal models (Shao et al., 2021). The spine-growth data come from mouse prefrontal cortex; whether the same structural changes occur in humans and whether they causally drive the mood improvement seen in clinical trials is inferred from outcome data, not directly demonstrated.
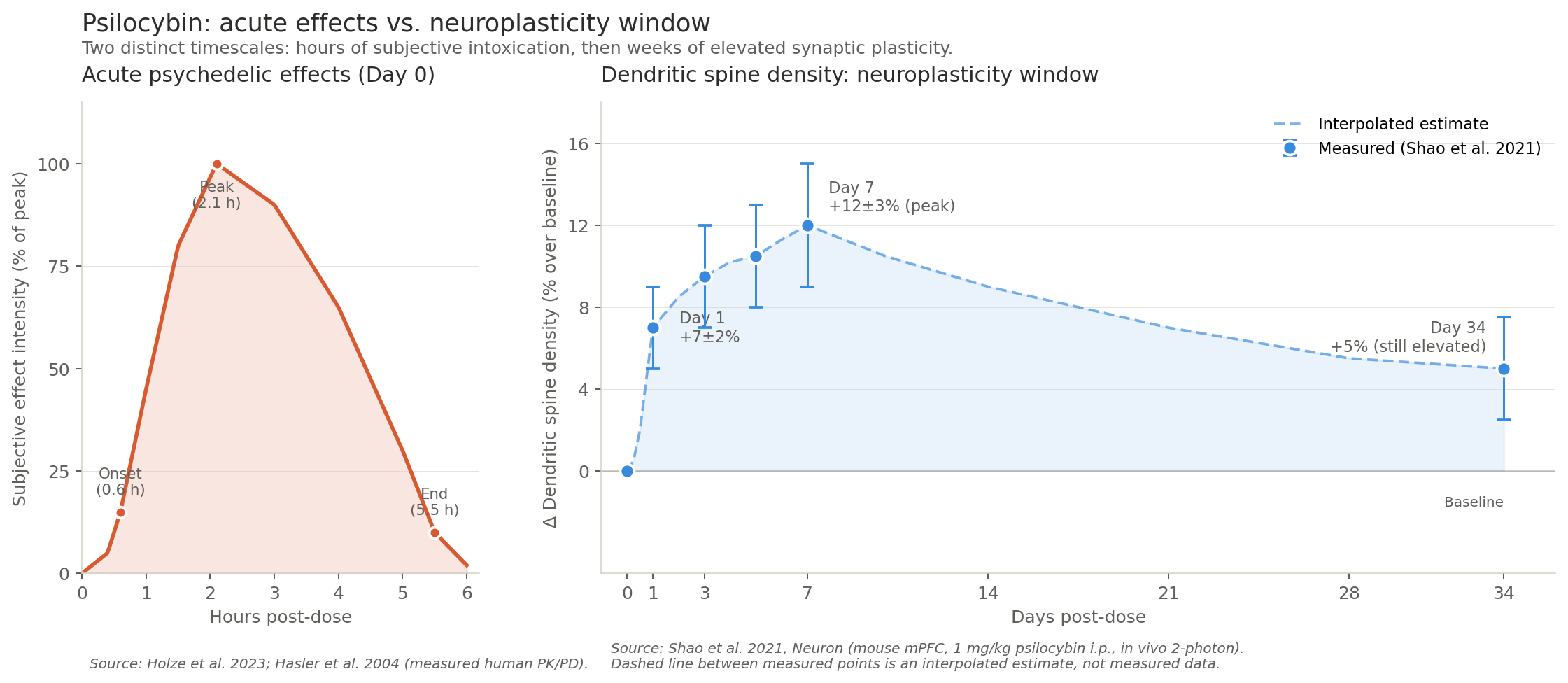
The result: a single dose of a psychedelic produces a window of increased synaptic plasticity that outlasts the drug itself by days to weeks.
This is mechanistically why:
- Mood improvement can persist for weeks after a single therapeutic dose.
- Psychedelics show effect in conditions characterized by "stuck" patterns of thinking - depression, addiction, PTSD.
- Therapeutic protocols pair the drug with psychotherapy during the plasticity window.
The plasticity window, not the trip itself, is the leading hypothesis for why therapeutic protocols work. Importantly, this plasticity does not appear to require ego dissolution to occur - the trip and the plasticity are related but separable. Non-hallucinogenic 5-HT2A agonists being developed may retain some plasticity benefit without the experience. Research is ongoing.
Step 10: Brain-Wide Consequences of the Trip
Once the receptors are activated and signaling pathways are running, effects propagate across networks. Three changes show up in neuroimaging across all classic psychedelics (Carhart-Harris & Friston, 2019):
- DMN desynchronization. The Default Mode Network normally maintains the sense of "I am separate from the world." Under psychedelics, the DMN's internal connectivity drops. Self-related circuits decouple. This produces ego dissolution.
- Visual cortex α-oscillation suppression (when Gq-mediated cortical excitation dominates). V1 normally uses α-oscillations to filter internally-generated activity from external visual input. Strong 5-HT2A/Gq activation suppresses α-power → external visual input loses dominance → the brain "sees" its own predictions.
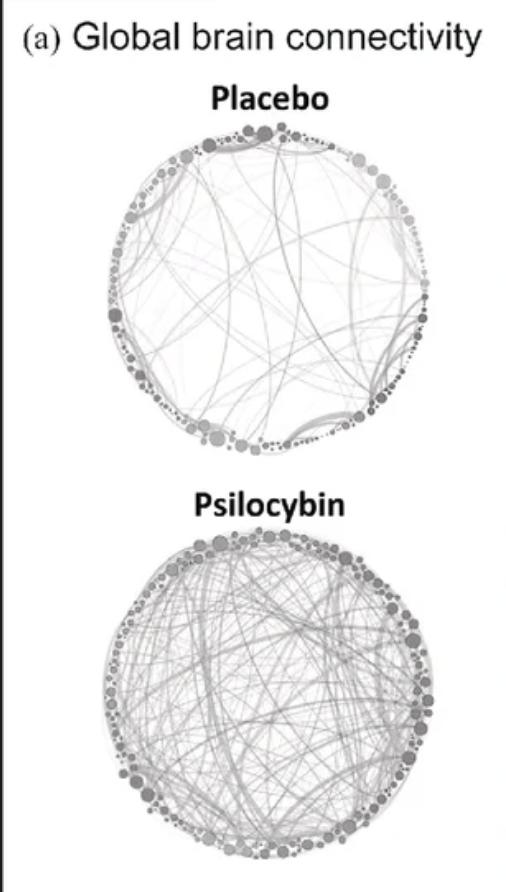
- Increased cross-region connectivity. Brain regions that don't normally communicate begin exchanging signals - the "entropy" picture of the psychedelic brain.
The Balancing Loop - Tachyphylaxis
Classic psychedelics produce rapid tachyphylaxis. Driven by (Buchborn et al., 2018):
- β-arrestin2 recruitment to the activated 5-HT2A receptor.
- Receptor internalization - the receptor is pulled inside the cell.
- Downregulation of available surface 5-HT2A density.

The brain simply stops responding, with no chemical drive to redose. Dopamine release is not central to the experience, so there is no sustained reward-circuit activation driving compulsive use. This is why classic psychedelics do not produce physical dependence.
User Manual
Specific Risks
- Persistent psychotic disorders in vulnerable individuals. Personal or family history of schizophrenia or bipolar I is a contraindication. Strong 5-HT2A agonism in a predisposed brain can trigger lasting episodes.
- Hallucinogen Persisting Perception Disorder (HPPD). Visual disturbances persisting after acute effects, sometimes for years. Risk is low but real and unpredictable - cannot be screened for in advance.
- Acute behavioral risk from severely impaired judgment during the trip.
- Acute cardiovascular events in users with pre-existing heart disease, uncontrolled hypertension, or arrhythmias. The 5-HT2A-driven sympathetic surge is well-tolerated in healthy users but unsafe in vulnerable ones.
- Hyperthermia in hot environments, especially with prolonged physical activity. Same hypothalamic mechanism as MDMA but typically milder.
- Valvular heart disease with chronic frequent dosing - mediated by 5-HT2B. Acute single use is not the concern; high-frequency microdosing protocols may warrant caution.
- Serotonin syndrome if combined with MAOIs (especially in ayahuasca contexts) or, rarely, with high-dose SSRIs.
- Research chemicals sold as psychedelics. "LSD" tabs are sometimes 25I-NBOMe or other NBOMe compounds, which have narrower therapeutic windows, can cause seizures, hypertensive crisis, and death at recreational doses. Reagent testing distinguishes them.
Therapeutic research is active. Psilocybin, LSD, and DMT are being studied for treatment-resistant depression, end-of-life anxiety, addiction, and PTSD, with FDA breakthrough therapy designations for some indications. This is mechanistically supported by the neuroplasticity effects covered in Step 9.
User Manual
- Set and setting are part of the pharmacology - trusted sober sitter, low-stimulus environment.
- Stay cool, hydrate appropriately, but do not overdrink water. Hyponatremia (dilutional low sodium) has been reported with psychedelics and MDMA, particularly when users drink large amounts of plain water. Sip, don't chug.
- Avoid extreme physical exertion.
- Do not combine with lithium (seizure risk) or tramadol.
- Trip-killers exist and work: benzodiazepines and antipsychotics both terminate a trip in minutes. Do not use benzodiazepines as a trip-killer if significant alcohol or other CNS depressants are also on board - adding a benzo on top of depressants risks respiratory depression. In that case, antipsychotics are safer. Medical help is the right call if a bad trip is escalating.
- Test substances - NBOMes sold as LSD are categorically more dangerous than LSD itself.
- If considering a sustained microdosing protocol, the 5-HT2B cardiac question is worth taking seriously.
After any break from psychedelics, tolerance resets completely within 1–2 weeks. The dose that felt manageable previously will feel much stronger again.
Sources
- Buchborn, T., et al. (2018). Tolerance and tachyphylaxis to head twitches induced by the 5-HT2A agonist 25CN-NBOH. Frontiers in Pharmacology, 9, 17. https://doi.org/10.3389/fphar.2018.00017
- Carhart-Harris, R. L., et al. (2016). Neural correlates of the LSD experience revealed by multimodal neuroimaging. PNAS, 113(17), 4853–4858. https://doi.org/10.1073/pnas.1518377113
- Carhart-Harris, R. L., & Friston, K. J. (2019). REBUS and the anarchic brain. Pharmacological Reviews, 71(3), 316–344. https://doi.org/10.1124/pr.118.017160
- Halberstadt, A. L., & Geyer, M. A. (2011). Multiple receptors contribute to the behavioral effects of indoleamine hallucinogens. Neuropharmacology, 61(3), 364–381. https://doi.org/10.1016/j.neuropharm.2011.01.017
- Hasler, F., Grimberg, U., Benz, M. A., Huber, T., & Vollenweider, F. X. (2004). Acute psychological and physiological effects of psilocybin in healthy humans: a double-blind, placebo-controlled dose-effect study. Psychopharmacology, 172(2), 145–156. https://doi.org/10.1007/s00213-003-1640-6
- Holze, F., Becker, A. M., Kolaczynska, K. E., Duthaler, U., & Liechti, M. E. (2023). Pharmacokinetics and pharmacodynamics of oral psilocybin administration in healthy participants. Clinical Pharmacology & Therapeutics, 113(4), 822–831. https://doi.org/10.1002/cpt.2821
- Hutcheson, J. D., et al. (2011). Serotonin receptors and heart valve disease - it was meant 2B. Pharmacology & Therapeutics, 132(2), 146–157. https://doi.org/10.1016/j.pharmthera.2011.03.008
- Kraehenmann, R., et al. (2015). Psilocybin-induced decrease in amygdala reactivity correlates with enhanced positive mood in healthy volunteers. Biological Psychiatry, 78(8), 572–581. https://doi.org/10.1016/j.biopsych.2014.04.010
- Ly, C., et al. (2018). Psychedelics promote structural and functional neural plasticity. Cell Reports, 23(11), 3170–3182. https://doi.org/10.1016/j.celrep.2018.05.022
- Madsen, M. K., et al. (2019). Psychedelic effects of psilocybin correlate with serotonin 2A receptor occupancy and plasma psilocin levels. Neuropsychopharmacology, 44(7), 1328–1334. https://doi.org/10.1038/s41386-019-0324-9
- Mechan, A. O., et al. (2002). The pharmacology of the acute hyperthermic response that follows administration of MDMA ("ecstasy") to rats. British Journal of Pharmacology, 135(1), 170–180. https://doi.org/10.1038/sj.bjp.0704442
- Neuroscientifically Challenged. (n.d.). 2-Minute neuroscience: Serotonin [Video]. YouTube. https://www.youtube.com/watch?v=Xkl_x6wC0Lg
- Nichols, D. E. (2016). Psychedelics. Pharmacological Reviews, 68(2), 264–355. https://doi.org/10.1124/pr.115.015212
- Roth, B. L. (2007). Drugs and valvular heart disease. New England Journal of Medicine, 356(1), 6–9. https://doi.org/10.1056/NEJMp068265
- Rothman, R. B., et al. (2000). Evidence for possible involvement of 5-HT2B receptors in the cardiac valvulopathy associated with fenfluramine and other serotonergic medications. Circulation, 102(23), 2836–2841. https://doi.org/10.1161/01.CIR.102.23.2836
- Shao, L.-X., Liao, C., Gregg, I., Davoudian, P. A., Savalia, N. K., Delagarza, K., & Kwan, A. C. (2021). Psilocybin induces rapid and persistent growth of dendritic spines in frontal cortex in vivo. Neuron, 109(16), 2535–2544.e4. https://doi.org/10.1016/j.neuron.2021.06.008
- Vargas, M. V., et al. (2023). Psychedelics promote neuroplasticity through the activation of intracellular 5-HT2A receptors. Science, 379(6633), 700–706. https://doi.org/10.1126/science.adf0435
- Wacker, D., et al. (2017). Crystal structure of an LSD-bound human serotonin receptor. Cell, 168(3), 377–389.e12. https://doi.org/10.1016/j.cell.2016.12.033
- Wallach, J., et al. (2023). Identification of 5-HT2A receptor signaling pathways associated with psychedelic potential. Nature Communications, 14(1), 6980. https://doi.org/10.1038/s41467-023-42579-7