Deliriants
Step 1: What the Drug Does
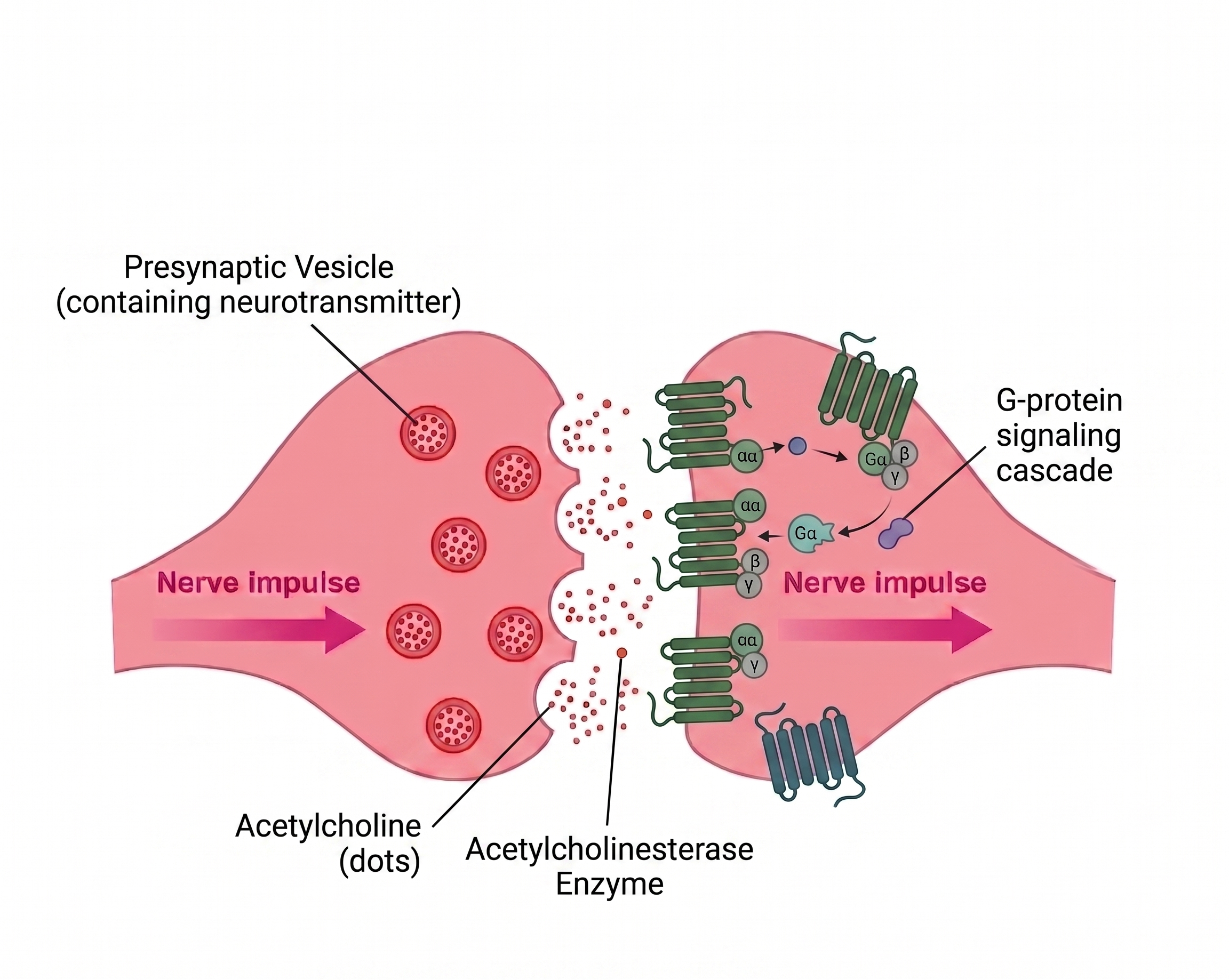
Deliriants are competitive antagonists at muscarinic acetylcholine receptors (mAChRs). They occupy the receptor without activating it, blocking endogenous acetylcholine from binding, so the cholinergic system goes dark.
There are five muscarinic subtypes (M1–M5), each in different tissues with different jobs. Most deliriants block all five non-selectively, which is why the symptom profile is so broad. The classical toxidrome comes mostly from M1, M2, and M3 blockade. The more recently appreciated psychiatric and reinforcing effects come from M4 and M5.
Mechanistically opposite to nicotine, which activates a different family of cholinergic receptors, the nicotinic ones. They share a neurotransmitter, not a mechanism.
One-line summary: Deliriants = "block acetylcholine signaling everywhere."
Step 2: What Acetylcholine Normally Does (via mAChRs)
ACh hitting muscarinic receptors does very different jobs depending on subtype and location (Eglen, 2006; Caulfield & Birdsall, 1998):
- M1 (CNS, mostly cortex and hippocampus) - memory consolidation, sensory gating (filtering relevant signals from noise), arousal regulation.
- M2 (heart, also presynaptic in CNS) - slows heart rate (vagal "brake"); presynaptically, autoreceptor function that regulates ACh release.
- M3 (smooth muscle and glands) - activates sweat glands, salivary glands, GI motility, pupillary constriction, bladder emptying.
- M4 (striatum, basal ganglia) - inhibits dopamine release. Acts as a "brake" on dopaminergic tone in the reward circuit (Threlfell et al., 2010; Bonsi et al., 2011).
- M5 (VTA, substantia nigra) - promotes dopamine release. The only muscarinic subtype expressed on midbrain dopamine neurons themselves - acts as the "accelerator" on dopaminergic tone (Foster et al., 2014; Yeomans, 1995).
The M4/M5 balance. In the reward circuit, M4 and M5 work in opposition: M4 dampens dopamine release, M5 promotes it. Resting cholinergic tone keeps both engaged at low levels. Block them both → dopamine signaling is disrupted in a complex way that depends on which receptor was contributing more at baseline. (Some people hate it, some people love it - but most people hate it, so don't do these, they suck.)
Step 3: Where mAChRs Live

Step 4: How Side Effects Fall Out of Steps 1–3
This is the anticholinergic toxidrome; clinicians remember it as: blind as a bat, mad as a hatter, red as a beet, hot as a hare, dry as a bone. Each piece maps to blocking a specific muscarinic job in a specific region (Broderick et al., 2023).
Classical Peripheral and CNS Toxidrome (M1, M2, M3)
"mad as a hatter"
"hot as a hare," "dry as a bone"
"blind as a bat"
"red as a beet"
Dopaminergic Effects (M4, M5)
Blocking M4 and M5 simultaneously creates a tug-of-war in the reward circuit. The net effect depends on regional balance and dose, but the documented consequences include:
M4 agonists are now in late-stage clinical trials as a new class of antipsychotic - they reduce dopamine release in the mesolimbic pathway without the metabolic side effects of D2 blockers (Kaul et al., 2024; xanomeline-trospium / KarXT). M4 agonism reduces psychosis; by symmetry, M4 antagonism - what deliriants do - pushes toward psychosis-like states. The delirium is not just M1 sensory-gating failure; it has a dopaminergic component.
True Hallucinations vs. Psychedelic Hallucinations
Critical distinction. Psychedelic users typically know they are having visual distortions. Deliriant users fully believe their hallucinations are real - conversations with people who aren't there, smoking cigarettes that don't exist, believing they've gone home when they're still on the floor. This is qualitatively different and clinically much more dangerous.
The mechanism: deliriants break the sensory-gating system (M1 in hippocampus and cortex) that distinguishes internal signals from external reality, and simultaneously disrupt dopaminergic-cortical communication (M4/M5) that normally tags experiences with the right reality-status. The brain has no way to flag the hallucinations as not-real because both the perceptual filter and the reality-monitoring system are offline.
The Balancing Loop
Chronic muscarinic blockade → compensatory upregulation of mAChR density across all subtypes. Sudden discontinuation → cholinergic rebound:
- Hypersalivation
- Bradycardia
- GI cramps
- Severe REM sleep rebound: intense, vivid nightmares
- Anxiety and irritability driven by the rebound in M4/M5 dopaminergic balance
User Manual
No established recreational dose; plant alkaloid concentrations vary enormously between specimens. Hallucinations are indistinguishable from reality, often leading to dangerous behavior: walking into traffic, falling from heights, attempting to "rescue" hallucinated family members. Effects can last 24–72 hours.
Two observations that M1 sensory-gating failure alone does not account for:
- Why deliriants have measurable abuse potential despite being subjectively unpleasant - diphenhydramine misuse is a documented clinical entity, particularly among adolescents.
- Why deliriant intoxication looks more like psychosis than like a classic hallucinogenic experience - the dopamine dysregulation pushes the experience toward psychotic-spectrum phenomenology rather than perceptual distortion alone.
(If you are dependent on deliriants, please seek professional help, as these carry serious long-term cognitive risks.)
If exposure has occurred (intentional or accidental), seek medical attention. Physostigmine (a cholinesterase inhibitor used in hospital settings, with its own risk profile) reverses anticholinergic toxicity in severe cases by raising synaptic acetylcholine high enough to outcompete the blocker at the receptor. Sober supervision is essential - users cannot reliably distinguish hallucinations from reality. Chronic use of anticholinergic drugs (including over-the-counter sleep aids and allergy medications) is associated with increased dementia risk in older adults; this is now a recognized clinical concern. Paradoxically, the muscarinic antagonist scopolamine has been investigated as a rapid-acting antidepressant at sub-anesthetic doses (Furey & Drevets, 2006).
Sources
- Bonsi, P., et al. (2011). Centrality of striatal cholinergic transmission in basal ganglia function. Frontiers in Neuroanatomy, 5, 6. https://doi.org/10.3389/fnana.2011.00006
- Broderick, E. D., et al. (2023). Anticholinergic toxicity. StatPearls Publishing. https://www.ncbi.nlm.nih.gov/books/NBK534798/
- Cancelli, I., et al. (2008). Drugs with anticholinergic properties: cognitive and neuropsychiatric side-effects in elderly patients. Neurological Sciences, 29(Suppl 1), S73–S80. https://doi.org/10.1007/s10072-008-0901-x
- Caulfield, M. P., & Birdsall, N. J. (1998). International Union of Pharmacology. XVII. Classification of muscarinic acetylcholine receptors. Pharmacological Reviews, 50(2), 279–290. https://pharmrev.aspetjournals.org/content/50/2/279
- Coupland, C. A. C., et al. (2019). Anticholinergic drug exposure and the risk of dementia: a nested case-control study. JAMA Internal Medicine, 179(8), 1084–1093. https://doi.org/10.1001/jamainternmed.2019.0677
- Eglen, R. M. (2006). Muscarinic receptor subtypes in neuronal and non-neuronal cholinergic function. Autonomic & Autacoid Pharmacology, 26(3), 219–233. https://doi.org/10.1111/j.1474-8673.2006.00368.x
- Foster, D. J., et al. (2014). M5 receptor activation produces opposing physiological outcomes in dopamine neurons depending on the receptor's location. Journal of Neuroscience, 34(9), 3253–3262. https://doi.org/10.1523/JNEUROSCI.4896-13.2014
- Foster, D. J., et al. (2021). Muscarinic acetylcholine receptors as novel treatment targets for schizophrenia. Pharmacological Reviews, 73(4), 1322–1339. https://doi.org/10.1124/pharmrev.120.000208
- Furey, M. L., & Drevets, W. C. (2006). Antidepressant efficacy of the antimuscarinic drug scopolamine. Archives of General Psychiatry, 63(10), 1121–1129. https://doi.org/10.1001/archpsyc.63.10.1121
- Halpert, A. G., et al. (2008). Behavioral effects of cyclopentolate and diphenhydramine in humans. Drug and Alcohol Dependence, 95(1–2), 145–155. https://doi.org/10.1016/j.drugalcdep.2008.01.005
- Kaul, I., et al. (2024). Efficacy and safety of xanomeline-trospium chloride in schizophrenia: a randomized clinical trial. The Lancet, 403(10422), 160–170. https://doi.org/10.1016/S0140-6736(23)02190-6
- Thomas, A., et al. (2009). Diphenhydramine abuse and detoxification: a brief review and case report. Journal of Psychopharmacology, 23(1), 101–105. https://doi.org/10.1177/0269881107083809
- Threlfell, S., et al. (2010). Striatal muscarinic receptors promote activity dependence of dopamine transmission via distinct receptor subtypes on cholinergic interneurons in ventral versus dorsal striatum. Journal of Neuroscience, 30(9), 3398–3408. https://doi.org/10.1523/JNEUROSCI.5620-09.2010
- Yeomans, J. S. (1995). Role of tegmental cholinergic neurons in dopaminergic activation, antimuscarinic psychosis and schizophrenia. Neuropsychopharmacology, 12(1), 3–16. https://doi.org/10.1016/0893-133X(94)00054-4