Empathogens (MDMA)
Step 1: What the Drug Does
MDMA is a serotonin substrate. It enters the presynaptic neuron via SERT (the serotonin transporter), then enters vesicles via VMAT2 and disrupts the proton gradient, dumping stored serotonin into the cytoplasm. The high cytoplasmic concentration then drives SERT into reverse, pushing serotonin out into the synaptic cleft. This is the same mechanism amphetamine uses on DAT, applied here to serotonin.
Secondarily, MDMA does the same to DAT and NET (the dopamine and norepinephrine transporters), but with lower affinity, producing some classical stimulant effects, like a weaker amphetamine layered on top.
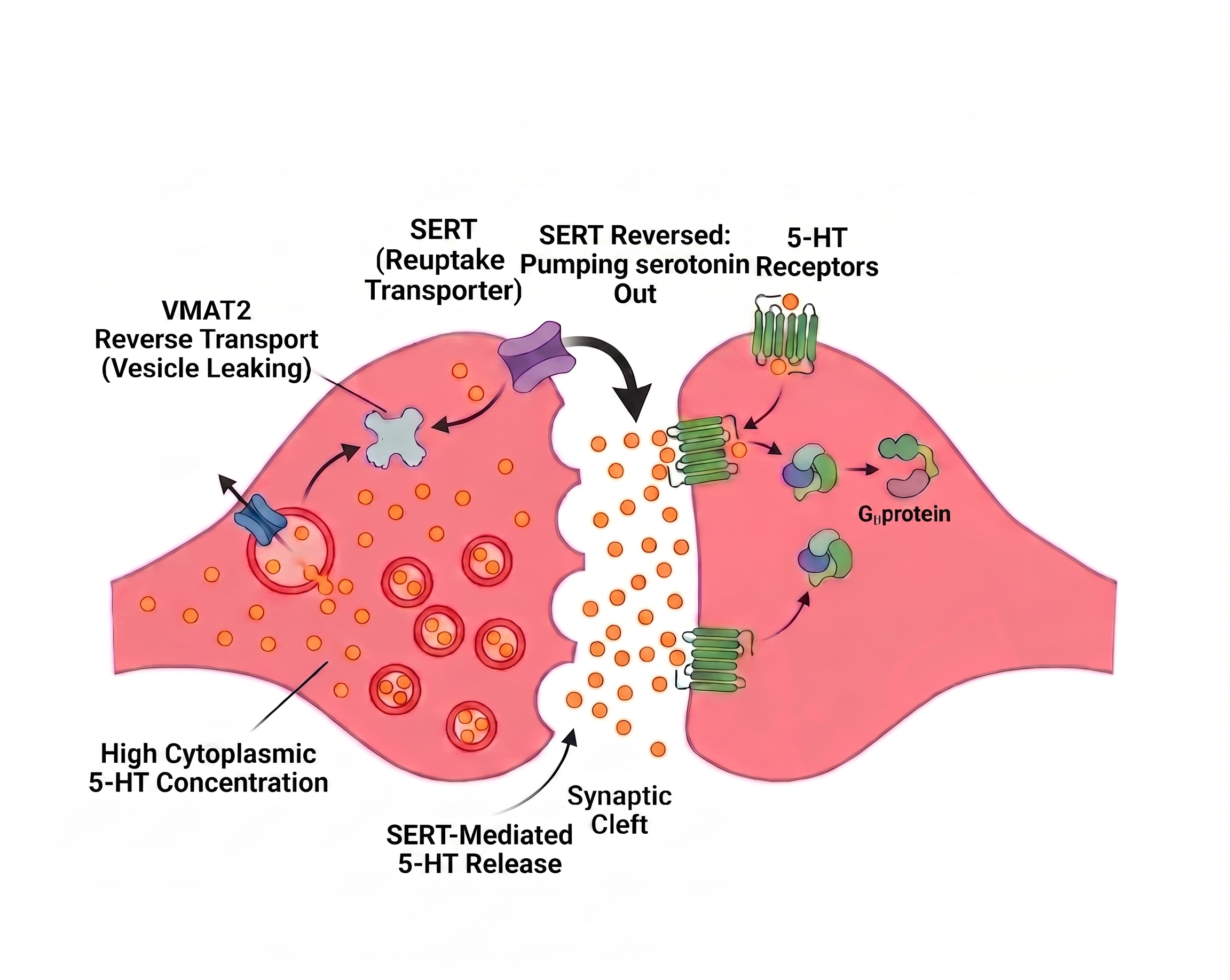
One-line summary: MDMA = "drives mass release of stored serotonin from presynaptic neurons into the synapse."
Step 2: What Serotonin Normally Does
Serotonin regulates mood, social behavior, fear processing, body temperature, and water balance. It is released in small, controlled amounts. There are at least 14 subtypes of 5-HT receptor scattered across the brain and body, each doing different things.
The relevant ones here:
- 5-HT receptors in amygdala - fear modulation
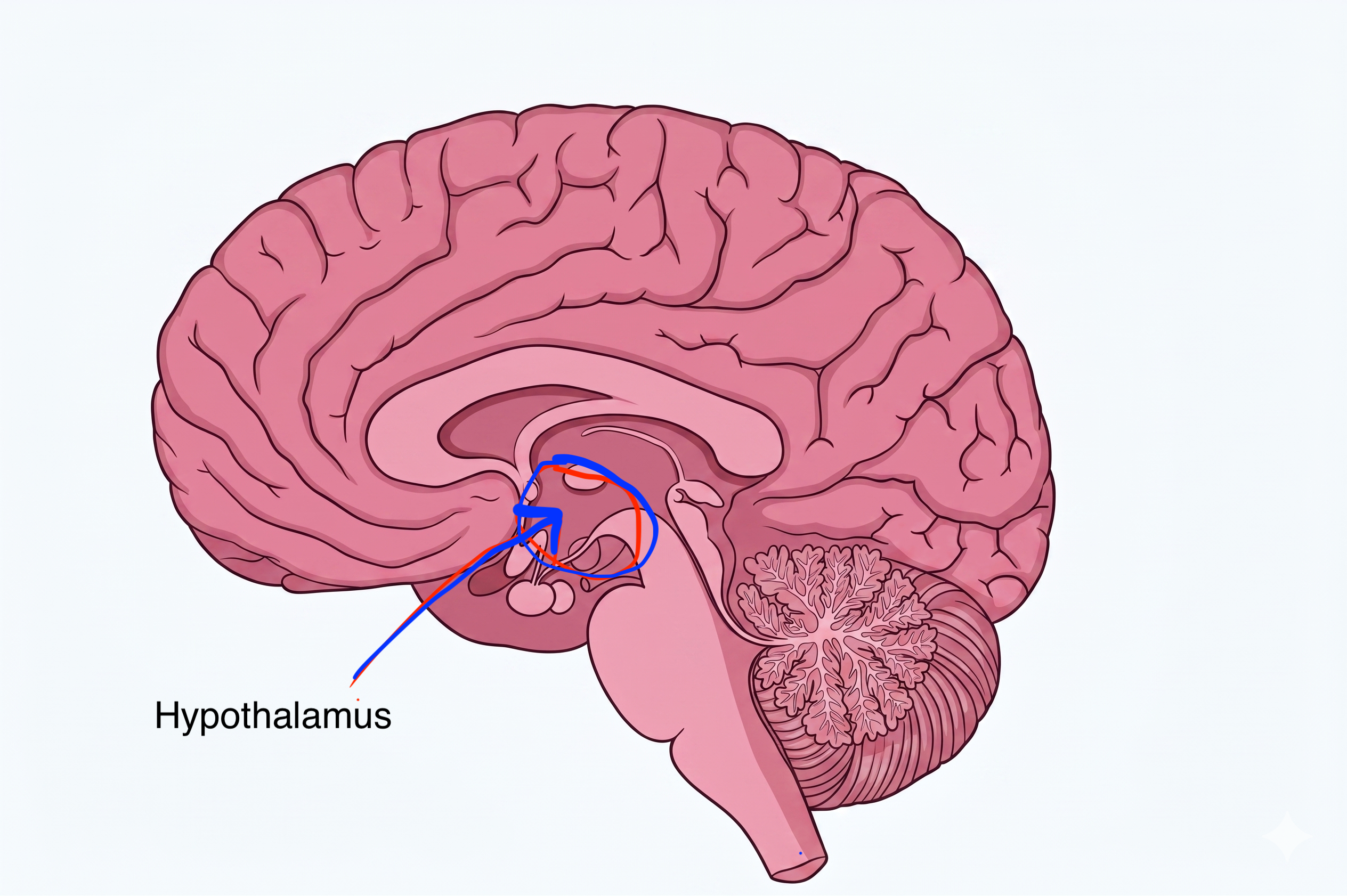
- 5-HT receptors in hypothalamus - hormone release (oxytocin, vasopressin) and thermoregulation
- 5-HT receptors throughout cortex - sensory and emotional processing
The same signal (serotonin) does very different things depending on where it lands. MDMA raises serotonin at all of these sites simultaneously; effects range from emotional warmth to dangerous overheating to brain swelling.
Step 3: Where MDMA-Released Serotonin Goes
 and Nucleus Raphe Magnus (Pain img).png)
 img.png)
Step 4: How Side Effects Fall Out of Steps 1–3
Each side effect follows directly from elevated serotonin acting on a specific region that normally receives serotonin in measured doses.
Empathy, Openness, Emotional Connection
Amygdala fear-processing neurons normally activate during threat. Massive 5-HT influx damps amygdala activity; the fear response is suppressed, and the user can revisit difficult emotional material without the normal fear circuitry firing. Hypothalamic 5-HT also drives oxytocin release, producing trust and bonding feelings. This is the basis of MDMA's therapeutic promise for PTSD (Mitchell et al., 2021).
↓
Hyperthermia
Hypothalamic 5-HT receptors regulate the body temperature set-point. Elevated serotonin disrupts the set-point, raising core temperature (Liechti, 2014). Combined with peripheral vasoconstriction (heat can't escape), physical exertion (often dancing), and high ambient temperatures, this can become fatal hyperthermia. The drug provides no warning signal; users feel energetic, not hot.
.png) ↑
↑
Hyponatremia (Low Blood Sodium)
Hypothalamic 5-HT receptors trigger vasopressin (ADH) release (Forsling et al., 2002). Vasopressin signals the kidneys to retain water. Combined with drug-induced thirst and over-hydration (especially in club settings where users are told to "drink water"), blood sodium drops dangerously low. Severe hyponatremia causes brain swelling, seizures, and death. This has killed users who were actively trying to be safe.
↑
Bruxism (Jaw Clenching)
Serotonin and dopamine activation of the trigeminal motor system produces continuous jaw muscle activation signals, causing clenching and grinding. This is one of the most reliable physical signs of MDMA ingestion.
 ↑
↑
The Balancing Loop
MDMA's main dependency substrate is depletion, not classical receptor adaptation (as seen with opioids or dissociatives).
A typical dose empties presynaptic serotonin stores. Serotonin biosynthesis via tryptophan hydroxylase is slow - there is no shortcut. Until vesicular stores are rebuilt, normal serotonin signaling is mathematically impossible: the chemical simply isn't there.

Frequent MDMA use produces progressively worse comedowns and progressively weaker acute experiences; less serotonin is available to release each time. There is also evidence of long-term serotonergic neurotoxicity in heavy or frequent users (Capela et al., 2009), particularly when combined with hyperthermia.
User Manual
Spacing doses gives the serotonin system time to rebuild stores and recover from oxidative stress. Reducing frequency reduces both acute risk (dehydration, hyperthermia, hyponatremia) and chronic risk (neurotoxicity). The widely cited minimum is 6–12 weeks between doses; "3 months" is the conservative rounding of that range. The truly safe frequency is unknown.
Hyponatremia from over-hydration has killed MDMA users who were following "drink lots of water" harm-reduction advice. The correct guidance is to sip water: roughly 500 ml/hour if actively sweating, significantly less if sedentary, and to supplement electrolytes.
User Manual
- In a hot environment, take breaks: exit the dance floor, cool down. Hyperthermia builds silently.
- Sip water (~500 ml/hour max if sweating, less if sedentary). Supplement electrolytes. Do not chug.
- Test substances. "MDMA" sold today frequently contains other compounds including fentanyl analogues and novel cathinones with different risk profiles.
- Minimum spacing to reduce neurotoxicity risk is 6–12 weeks between doses. Truly safe frequency is unknown.
- Hyperthermia and hyponatremia are the primary acute killers, not the drug's direct pharmacology at normal doses.
Sources
- Capela, J. P., et al. (2009). Molecular and cellular mechanisms of ecstasy-induced neurotoxicity. Molecular Neurobiology, 39(3), 210–271. https://doi.org/10.1007/s12035-009-8064-1
- Forsling, M. L., et al. (2002). The effect of MDMA ('ecstasy') and its metabolites on neurohypophysial hormone release from the isolated rat hypothalamus. British Journal of Pharmacology, 135(3), 649–656. https://doi.org/10.1038/sj.bjp.0704539
- Liechti, M. E. (2014). Effects of MDMA on body temperature in humans. Temperature (Austin, Tex.), 1(3), 192–200. https://doi.org/10.4161/23328940.2014.955433
- Mitchell, J. M., et al. (2021). MDMA-assisted therapy for severe PTSD: a randomized, double-blind, placebo-controlled phase 3 study. Nature Medicine, 27(6), 1025–1033. https://doi.org/10.1038/s41591-021-01336-3