Dissociatives
Note on nitrous oxide: Nitrous appears in both this submodule and Module 6a: Inhalants. Mechanistically it is a dissociative - it acts as an NMDA channel blocker, but it is commonly grouped with inhalants because of how it is used and obtained. The mechanism here applies; the route-of-use context is in 6a.
Step 1: What the Drug Does
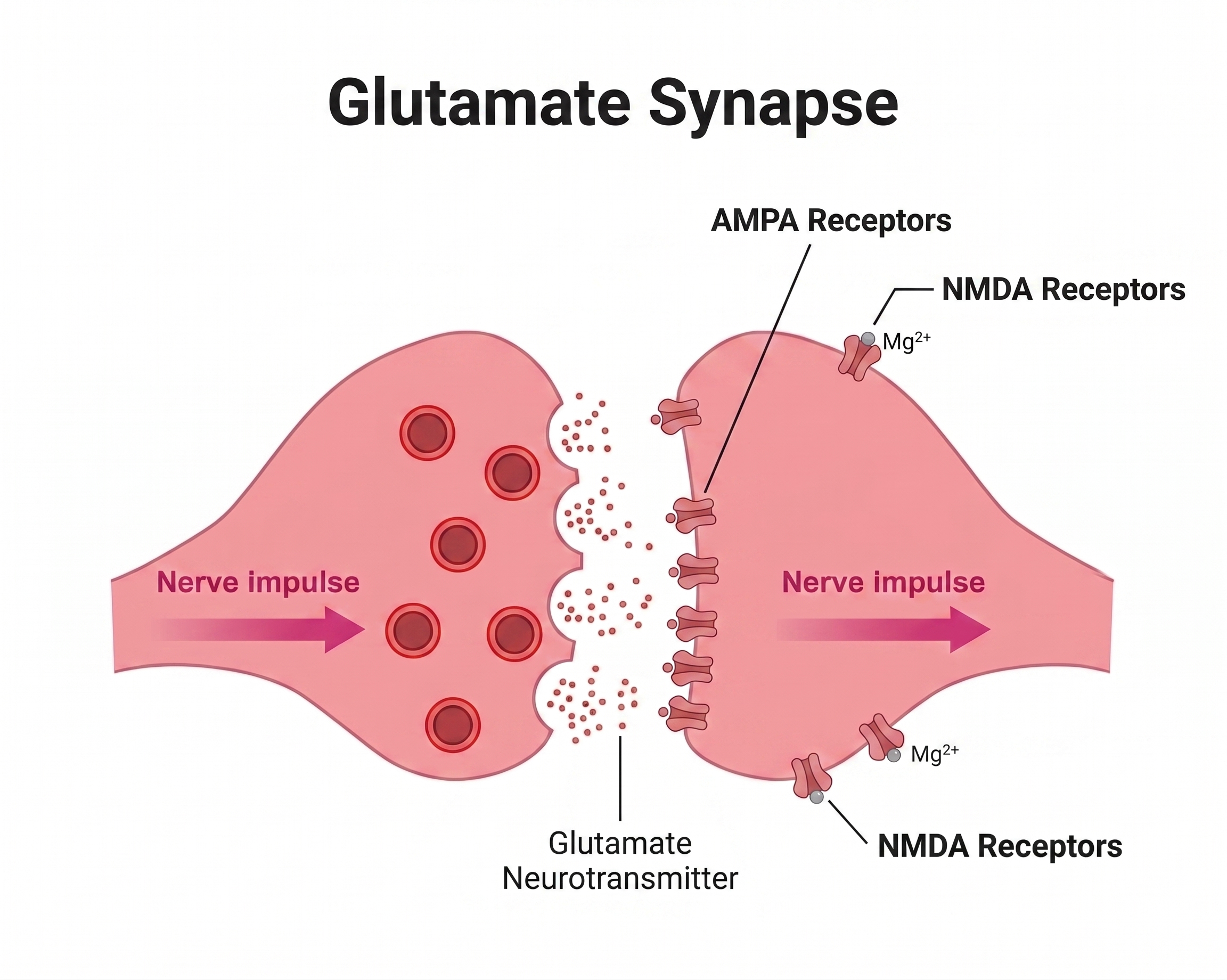
Dissociatives are non-competitive open-channel blockers at the NMDA receptor. They don't compete with glutamate at the binding site; they slip into the open channel pore and physically plug it. As long as the drug is bound, glutamate can bind all it wants, but Ca²⁺ cannot get in.
One-line summary: Dissociatives = "physically plug the brain's main excitatory channel."
Video: Ketamine - click to expand ↗ YouTube
Step 2: What NMDA Normally Does
Review: Glutamate is the brain's main excitatory neurotransmitter. NMDA is a special glutamate-gated channel that is also voltage-gated - at rest, a magnesium ion (Mg²⁺) sits in the pore blocking it. Only when the cell is already partially depolarized does the Mg²⁺ pop out, letting Ca²⁺ and Na⁺ flow in.
This Ca²⁺ influx drives long-term potentiation (LTP) (Paoletti et al., 2013). NMDA is also the main carrier of high-frequency information across networks (e.g., thalamus → cortex relays). Block NMDA → information transfer across the brain breaks down.
The Mg²⁺ block is why NMDA is called a "coincidence detector" - it only opens when glutamate is present and the cell is already active. Dissociatives enter the channel only when it's open.
Step 3: Where NMDA Lives
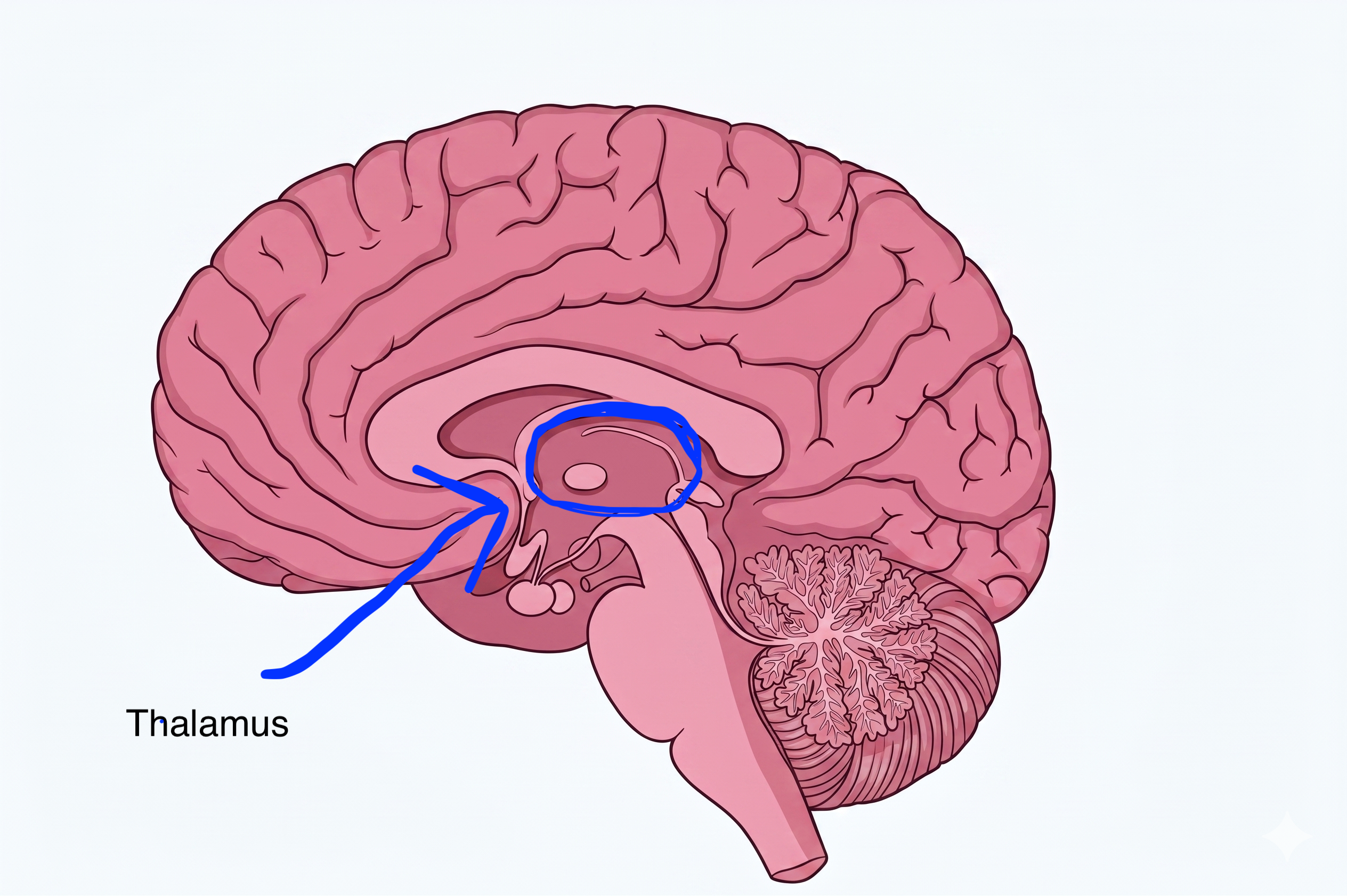
The thalamus is introduced here as a new region. It processes and routes nearly all sensory information (except smell) and motor signals to the cerebral cortex, the brain's central relay station.

 and Nucleus Raphe Magnus (Pain img).png)
Step 4: How Side Effects Fall Out
Each side effect follows directly from NMDA blockade in a specific region altering that region's normal job.
Dissociation / Out-of-Body Experience
The thalamus's job is to hand sensory data to the cortex via NMDA-dependent transmission. Block NMDA → thalamus can't deliver. Senses are working but the integration step has failed → depersonalization, derealization, "watching yourself from outside."
↓
Anterograde Amnesia
Hippocampal LTP requires NMDA Ca²⁺ influx. No Ca²⁺ = no LTP = no new memories formed. The "k-hole" is often partially or completely amnestic; the user is awake and moving but not encoding any of it.
↓
Analgesia and Anesthesia
Pain transmission in the spinal cord and PAG is NMDA-dependent. Block NMDA → pain signal can't propagate to cortex. Ketamine is a clinical anesthetic and is used for pain management in emergency medicine, interrupting the pain pathway at a mechanistic level.
↓
Cardiovascular - Paradoxical Increases
Ketamine is unusual in raising (rather than lowering) blood pressure and heart rate. Mechanism: cortical disinhibition from NMDA blockade releases noradrenergic tone → indirect sympathomimetic effect. Ketamine remains safe for anesthesia in patients in shock; most anesthetics drop blood pressure, but ketamine raises it.
 ↑
↑
Bladder Damage - Chronic Ketamine Only
"Ketamine cystitis." Severe, sometimes irreversible bladder inflammation and scarring. Mechanism: direct toxicity of ketamine and its metabolites on urothelial cells, not the NMDA mechanism. It does not generalize to other dissociatives in the same way. Risk is dose- and frequency-dependent; heavy daily users can lose significant bladder capacity.
 ↓
↓
The Balancing Loop
Chronic NMDA blockade → the cell upregulates NMDA receptor density to compensate. Drug removed → too many excitatory channels are now available, and normal glutamate activates them at excess.
- Hyperalgesia - paradoxical pain sensitivity, the opposite of the drug's effect.
- Excitotoxicity - uncontrolled Ca²⁺ influx from over-expressed NMDA receptors damages neurons.
- Cognitive impairment - disrupted NMDA signaling underlies working memory and executive function deficits seen in heavy users.

User Manual
Sub-anesthetic ketamine has rapid antidepressant effects (via mechanisms involving prefrontal cortex disinhibition and BDNF release; Krystal et al., 1994; Zanos & Gould, 2018) and is now used clinically (esketamine/Spravato, IV ketamine infusions). Recreational use of the same drug at higher doses risks bladder damage, dependency, and cognitive impairment. The dose-response curve matters enormously here: therapeutic ketamine and recreational ketamine are different experiences with different risk profiles, even though it's the same molecule.
Chronic recreational ketamine use carries real risk of bladder damage that may be irreversible. Case series have documented bladder shrinkage requiring surgical intervention in heavy daily users; the threshold for damage is not precisely established, but risk scales with dose and frequency (Niesters et al., 2014). This damage is not reversible once it progresses far enough.
User Manual
- Don't use dissociatives near water; drowning risk during disconnection from reality is real and well-documented.
- Don't combine with depressants; both suppress breathing through different mechanisms, and the combination has no ceiling effect warning.
- Chronic recreational ketamine use has a dose-dependent bladder toxicity risk that is distinct from any other dissociative in this list.
- The k-hole is not dangerous by itself in a safe environment; it becomes dangerous when the user is mobile, near hazards, or alone.
- Never use dissociatives alone. The k-hole produces complete dissociation from reality and inability to call for help. Have a sober person present.
Sources
- Krystal, J. H., et al. (1994). Subanesthetic effects of the noncompetitive NMDA antagonist, ketamine, in humans. Archives of General Psychiatry, 51(3), 199–214. https://doi.org/10.1001/archpsyc.1994.03950030007002
- Neuroscientifically Challenged. (n.d.). 2-Minute neuroscience: Ketamine [Video]. YouTube. https://www.youtube.com/watch?v=kRtNsaMildw
- Niesters, M., et al. (2014). Ketamine for chronic pain: risks and benefits. British Journal of Clinical Pharmacology, 77(2), 357–367. https://doi.org/10.1111/bcp.12164
- Paoletti, P., et al. (2013). NMDA receptor subunit diversity: impact on receptor properties, synaptic plasticity and disease. Nature Reviews Neuroscience, 14(6), 383–400. https://doi.org/10.1038/nrn3504
- Zanos, P., & Gould, T. D. (2018). Mechanisms of ketamine action as an antidepressant. Molecular Psychiatry, 23(4), 801–811. https://doi.org/10.1038/mp.2017.255