Caffeine
Step 1: What the Drug Does
Caffeine is an adenosine receptor antagonist. It competes with adenosine for the same binding sites and blocks the signal without activating the receptor.
- A1 blockade → neurons that adenosine was quieting fire freely again → general alertness, reduced fatigue.
- A2A blockade → sleep pressure signal blocked, and because A2A normally opposes dopamine D2, blocking A2A indirectly lets dopamine signaling rise → mild mood lift, the faint "reward" of caffeine.
One-line summary: Caffeine = "blocks the brain's own tiredness signal at its receptor."
Video: Caffeine and Adenosine Receptors - click to expand ↗ YouTube
Step 2: What Adenosine Normally Does
Where Adenosine Comes From
Every cell runs on ATP (adenosine triphosphate), the molecule that stores and delivers energy. When a cell does work, it spends ATP, breaking it down step by step: ATP → ADP → AMP → and eventually adenosine (Boison, 2011).
The more work a neuron has done, the more ATP it has burned, and the more adenosine accumulates. Adenosine leaves the cell and builds up in the extracellular space. Its levels climb steadily over the day, encoding how long and how hard the brain has been working.
The Adenosine Receptors
Adenosine, once outside the cell, binds to adenosine receptors, which are G-protein-coupled receptors. Four subtypes exist (A1, A2A, A2B, A3); two matter here:
- A1 receptors - inhibitory. Found throughout the brain. When adenosine binds A1, the neuron is quieted (reduces cAMP, hyperpolarizes the cell). A1 activation broadly slows brain activity.
- A2A receptors - concentrated in the striatum and the brain's sleep-regulating regions. A2A activation promotes sleep pressure directly and also dampens dopamine signaling - A2A and dopamine D2 receptors sit together on striatal neurons and oppose each other (Ferré, 2008; Huang et al., 2005).
As adenosine accumulates through the day, it occupies more and more A1 and A2A receptors. Neurons fire less. Dopamine signaling is damped. The subjective result is drowsiness, the body's signal that it is time to sleep and recover (Ribeiro & Sebastião, 2010).
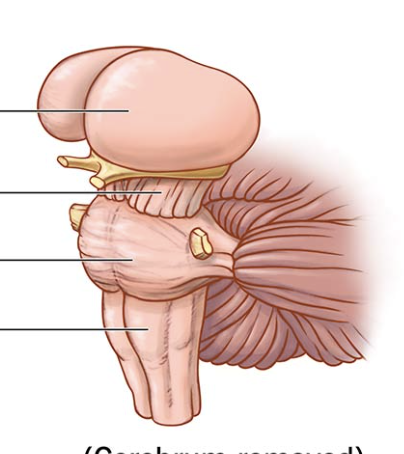
Step 3: Where Adenosine Receptors Live
Each region's normal job is what gets altered when caffeine blocks its adenosine receptors.
 ↑
↑ ↓
↓ ↑
↑ ↓
↓ ↑
↑ ↑
↑Striatum defined: the largest subcortical structure of the basal ganglia. It integrates cortical input and helps regulate movement, motivation, and reward - which is why A2A blockade there produces dopamine-linked mood effects.
Step 4: How the Effects Fall Out
Alertness, Reduced Fatigue
A1 and A2A blockade across the cortex and sleep centers hides the tiredness signal. Neurons that were being quieted by adenosine fire freely again.
↑
Mild Mood Lift, Mild Reinforcement
A2A blockade in the striatum disinhibits dopamine. This is also why caffeine is mildly habit-forming. There is a small dopamine component, though far weaker than the drugs in Module 5.
↑
Jitteriness, Anxiety at High Doses
With adenosine's quieting effect removed brain-wide, neurons across many circuits fire more. In excess this tips into tremor, anxiety, and racing thoughts.
↑
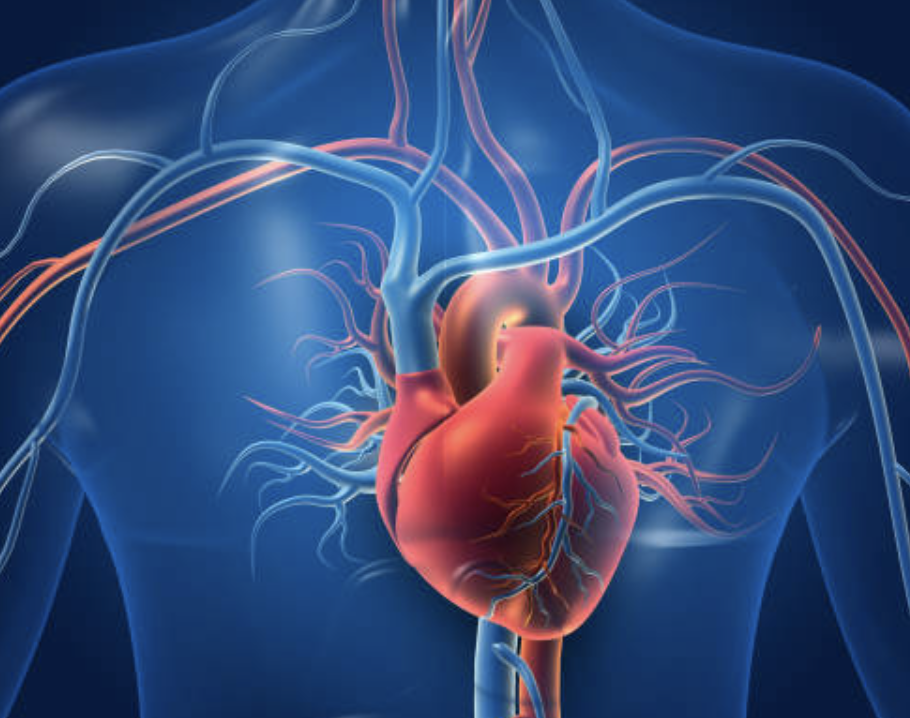
Effects on the Heart
Adenosine is one of the heart's natural brakes. A1 activation slows heart rate and conduction. (This is so reliable that pure adenosine is used as an emergency drug to stop certain abnormal fast heart rhythms.) Caffeine blocks cardiac A1 receptors → removes that brake → heart rate can rise. Caffeine also triggers a modest release of adrenaline, adding further cardiovascular stimulation. At high doses, in sensitive individuals, or in people with existing heart rhythm problems: palpitations, arrhythmia, blood pressure spikes. Caffeine also transiently increases aortic stiffness, contributing to the blood pressure response (Vlachopoulos et al., 2005).
↑
Effects on the Kidneys
The kidneys filter blood, and adenosine helps regulate that filtration. Caffeine blocking renal adenosine receptors does two things: increased filtration and urine output (caffeine is a mild diuretic; Marx et al., 2016), and sodium and water loss. Over a day of heavy intake this contributes to mild dehydration if fluids aren't replaced, though regular users develop partial tolerance to the diuretic effect.
↑
The Balancing Loop
Caffeine tolerance uses the exact same receptor-adaptation logic as the other drug classes in this curriculum, just applied to a receptor being blocked rather than activated.
The brain notices that its adenosine receptors are being chronically occupied by caffeine and that the tiredness signal is not getting through. To restore the signal, it builds more adenosine receptors, upregulating A1 (and A2A) receptor density so the adenosine that is present has more places to bind.

- Tolerance. With more adenosine receptors built, the same dose of caffeine blocks a smaller fraction. The adenosine present can still bind to the extras. The effect fades - the regular user needs caffeine just to feel normal.
- Withdrawal. Stop caffeine and all those upregulated receptors are suddenly unblocked. Now there is more adenosine receptor capacity than a non-user ever had, and the day's accumulating adenosine floods onto all of it. The result is an exaggerated tiredness signal: headache (adenosine dilating cerebral blood vessels - the reverse of caffeine's constriction; Sawynok, 2011), fatigue, low mood, difficulty concentrating, irritability. Peaks around 24–48 hours after the last dose, resolves over several days as the receptor count drifts back to baseline (Juliano & Griffiths, 2004).
The caffeine withdrawal headache is the clearest everyday example of the balancing-loop logic in this whole curriculum: block a receptor for long enough, the body builds more of it, and removing the block leaves the body over-supplied and over-signaling.
User Manual
Caffeine has a half-life of roughly 5 hours in healthy adults (Fredholm et al., 1999); this is extended significantly during pregnancy and by oral contraceptives, and shortened in smokers. A dose in the afternoon is still partly blocking adenosine receptors at bedtime, reducing sleep quality, which raises next-day adenosine and tiredness, which drives more caffeine use.
Sources
- Boison, D. (2011). Modulators of nucleoside metabolism in the therapy of brain diseases. Current Topics in Medicinal Chemistry, 11(8), 1068–1086. https://doi.org/10.2174/156802611795347609
- Ferré, S. (2008). An update on the mechanisms of the psychostimulant effects of caffeine. Journal of Neurochemistry, 105(4), 1067–1079. https://doi.org/10.1111/j.1471-4159.2007.05196.x
- Fredholm, B. B., et al. (1999). Actions of caffeine in the brain with special reference to factors that contribute to its widespread use. Pharmacological Reviews, 51(1), 83–133. https://pharmrev.aspetjournals.org/content/51/1/83
- Huang, Z. L., et al. (2005). Adenosine A2A, but not A1, receptors mediate the arousal effect of caffeine. Nature Neuroscience, 8(7), 858–859. https://doi.org/10.1038/nn1491
- Juliano, L. M., & Griffiths, R. R. (2004). A critical review of caffeine withdrawal: empirical validation of symptoms and signs, incidence, severity, and associated features. Psychopharmacology, 176(1), 1–29. https://doi.org/10.1007/s00213-004-2000-x
- Marx, B., et al. (2016). Mechanisms of caffeine-induced diuresis. Médecine Sciences, 32(5), 485–490. https://doi.org/10.1051/medsci/20163205015
- Ribeiro, J. A., & Sebastião, A. M. (2010). Caffeine and adenosine. Journal of Alzheimer's Disease, 20(S1), S3–S15. https://doi.org/10.3233/JAD-2010-1379
- Sawynok, J. (2011). Caffeine and pain. Pain, 152(4), 726–729. https://doi.org/10.1016/j.pain.2010.10.011
- Vlachopoulos, C., et al. (2005). Caffeine increases aortic stiffness in healthy subjects. American Journal of Hypertension, 18(1), 129–136. https://doi.org/10.1016/j.amjhyper.2004.08.030
- RCSB PDB. (n.d.). Caffeine and adenosine receptors [Video]. YouTube. https://www.youtube.com/watch?v=jOfquPE1cnU