Nicotine
To talk about nicotine we have to introduce the cholinergic system! Yippee. This was the first neurotransmitter to be discovered - at the muscle-to-neuron junction. Pretty cool.
This will be revisited in submodule 7c on muscarinic receptors!
Step 1: What the Drug Does
Video: Nicotine - click to expand ↗ YouTube
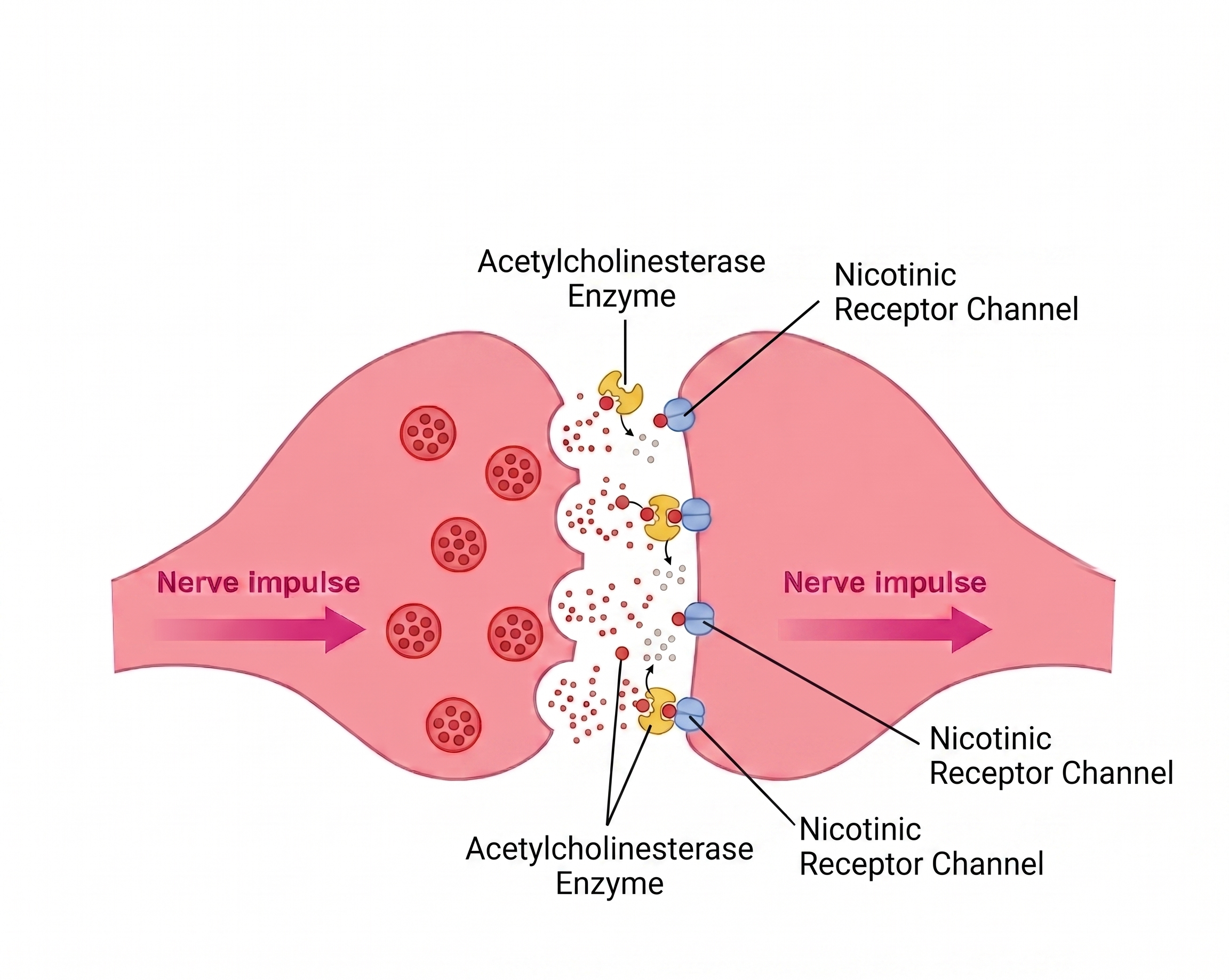
Acetylcholine (ACh) binds two distinct receptor families:
- Nicotinic (nAChRs) - fast ligand-gated ion channels
- Muscarinic (mAChRs) - slow G-protein coupled receptors
These two families share a neurotransmitter but do completely different things. Nicotine targets nAChRs; deliriants like Benadryl and datura target mAChRs as antagonists. Mechanistically opposite drugs, same neurotransmitter.
Nicotine mimics ACh at nicotinic acetylcholine receptors (nAChRs) - specifically the high-affinity α4β2 subtype, which is the receptor subtype most responsible for nicotine's reinforcing properties (Picciotto et al., 1998). These are ligand-gated ion channels: when nicotine binds, the channel opens and Na⁺ + Ca²⁺ flow in → depolarization → the neuron fires.
The twist: unlike acetylcholine, nicotine is not broken down by acetylcholinesterase. It stays bound. After initial activation, prolonged binding shoves the receptor into a closed, unresponsive state called desensitization.
One-line summary: Nicotine = fake acetylcholine that doesn't go away.
Step 2: What Acetylcholine Normally Does
ACh is the brain's main signal for attention, arousal, and learning. It is released during focus, novelty, and effortful cognition. The system is tightly regulated - ACh is quickly broken down by acetylcholinesterase to keep signals brief and precise.
This is why nerve agents (like sarin) are lethal: they irreversibly inhibit acetylcholinesterase, causing ACh to accumulate everywhere at once, triggering uncontrolled activation of every muscle, gland, and neuron in the body simultaneously.
Step 3: Where nAChRs Live

Step 4: How Side Effects Fall Out of Steps 1–3
Each side effect follows directly from nAChR activation in a specific region.
Note on diagrams: The dopamine and norepinephrine pathway images used in this section look similar and are used interchangeably - this is intentional. Both pathways share overlapping anatomy and the images are a simplification taken throughout this course.
Mild Stimulation, Focus, Mood Lift
VTA nAChR activation → dopamine release in NAc. LC nAChR activation → norepinephrine release → alertness and focus. This is a genuinely real pharmacological effect, not placebo. That's why nicotine persists as a drug despite its harm profile. It does something.
↑
Cardiovascular Effects
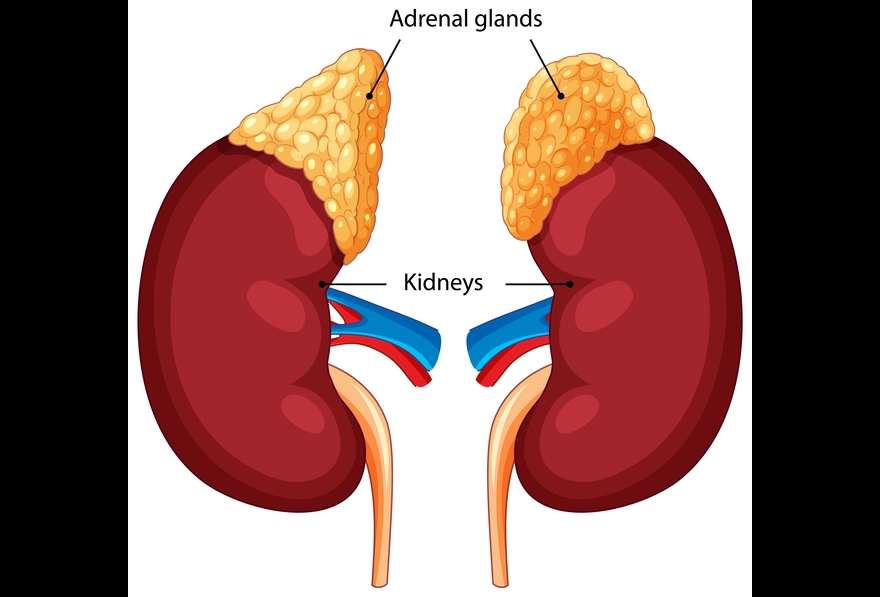
Adrenal medulla activation → systemic epinephrine release → tachycardia, transient blood pressure rise, peripheral vasoconstriction. Same mechanism as stimulant cardiovascular effects but milder. Chronic vasoconstriction is a significant contributor to smoking-related cardiovascular disease.
↑
Nausea / GI Effects
Parasympathetic ganglia activation → increased gut motility. Especially pronounced in first-time users who have no tolerance to peripheral nAChR activation.
 ↑
↑
The Balancing Loop
Most drugs cause receptor downregulation. Chronic nicotine causes receptor upregulation - but the mechanism is more nuanced than simple increased synthesis.
What's actually happening (Vallejo et al., 2005; Fenster et al., 1999):
- Nicotine pushes α4β2 receptors into the desensitized (non-functional) state.
- The cell senses a functional cholinergic deficit.
- Receptors get stabilized in a high-affinity conformation at the membrane. The increase in nicotine binding sites is partly a conformational shift, not just more protein synthesis.
- Net result: more α4β2 binding sites, but many sit desensitized while the drug is present.

Nicotine withdrawal is what happens when a brain tuned to constant nicotine signal tries to operate without it:
upregulated + sensitized receptors + normal ACh = hyperexcitable, anxious, dysphoric
So you smoke to get it back down to normal. It isn't more pleasurable. It's just getting back to normal.
User Manual
Nicotine delivered by inhalation is among the most rapidly addictive substances studied, comparable to or exceeding heroin and cocaine on dependence scales (Benowitz, 2010). Inhalation kinetics (lung-to-brain in ~7 seconds) combined with rapid receptor adaptation create an unusually tight addiction loop. Note: smoked tobacco also contains monoamine oxidase inhibitors (MAOIs) that potentiate nicotine's addictiveness further; pure nicotine products (patches, gum) are meaningfully less addictive, though still habit-forming. Vaping and pouches deliver pure nicotine at high doses and often increase total daily nicotine exposure relative to cigarettes.
During cessation, expect the worst of withdrawal in the first 72 hours. Significant craving continues for 2–4 weeks. Nicotine replacement (patch, gum, lozenge) and varenicline both work by giving the upregulated receptor pool something to stabilize on while the user tapers exposure down.
Sources
- Benowitz, N. L. (2010). Nicotine addiction. New England Journal of Medicine, 362(24), 2295–2303. https://doi.org/10.1056/NEJMra0809890
- Fenster, C. P., et al. (1999). Upregulation of surface α4β2 nicotinic receptors is initiated by receptor desensitization after chronic exposure to nicotine. Journal of Neuroscience, 19(12), 4804–4814. https://doi.org/10.1523/JNEUROSCI.19-12-04804.1999
- Neuroscientifically Challenged. (n.d.). 2-Minute neuroscience: Nicotine [Video]. YouTube. https://www.youtube.com/watch?v=I02WbuLiivw
- Picciotto, M. R., et al. (1998). Acetylcholine receptors containing the β2 subunit are involved in the reinforcing properties of nicotine. Nature, 391(6663), 173–177. https://doi.org/10.1038/34413
- Vallejo, Y. F., et al. (2005). Chronic nicotine exposure upregulates nicotinic receptors by a novel mechanism. Journal of Neuroscience, 25(23), 5563–5572. https://doi.org/10.1523/JNEUROSCI.5303-04.2005