Pharmacokinetics
How a drug moves through the body determines what it does. Same molecule, same milligrams, very different outcomes depending on route and timing.
3.1 Bioavailability (F): How Much Actually Arrives
Bioavailability = the percentage of a dose that reaches the bloodstream. Depends on the route.
- Oral - lowest. Drug passes through the liver before reaching the brain ("first-pass metabolism"). The liver destroys a major fraction.
- Snorted / under the tongue - largely bypasses the liver (some first-pass metabolism still occurs depending on drug and dose). Faster, more potent.
- Smoked / vaped - lungs to brain in seconds.
- Intravenous (IV) - 100%. No filters.
The dose to the brain can be 5–10× higher by a different route.
The speed of onset is one of the main indicators of addiction potential. Smoking something will be more addictive than eating it.
3.2 The Blood-Brain Barrier
The brain is sealed off from the bloodstream by a tight wall of cells. Only certain molecules pass.
- Fat-soluble (lipophilic) drugs - cross instantly.
- Water-soluble drugs - slow or blocked.
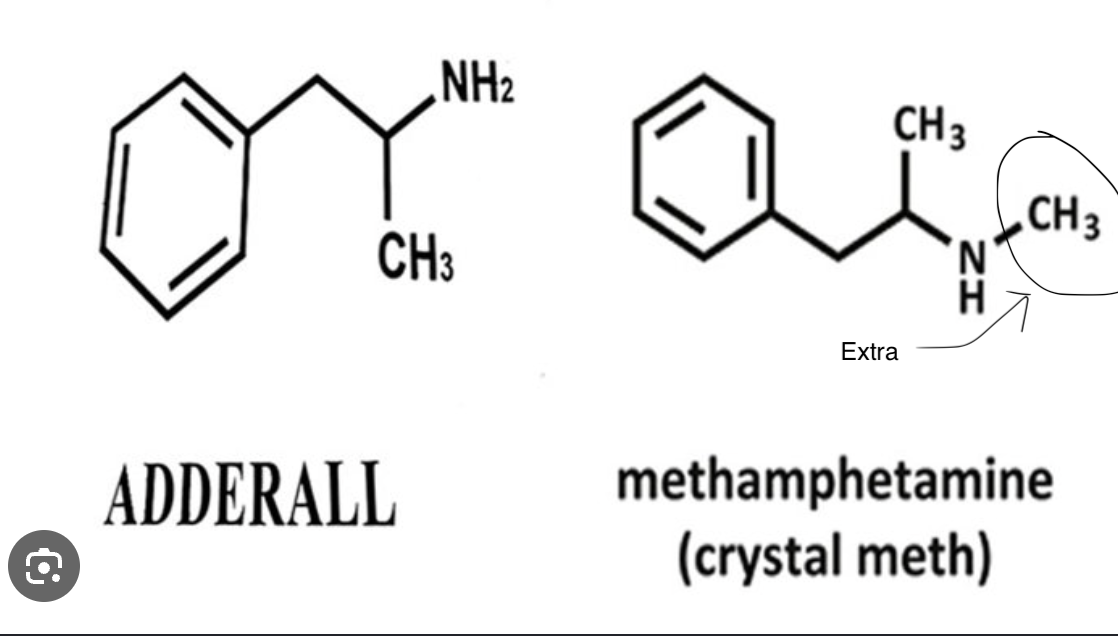
One key difference between meth and amphetamine (a key active ingredient in Adderall, which contains mixed amphetamine salts in a 75:25 dextro:levo ratio) is lipophilicity. Meth is more lipophilic, crossing the blood-brain barrier more easily and reaching the brain faster, contributing to its sharper subjective onset.
3.3 Half-Life vs. Active Duration
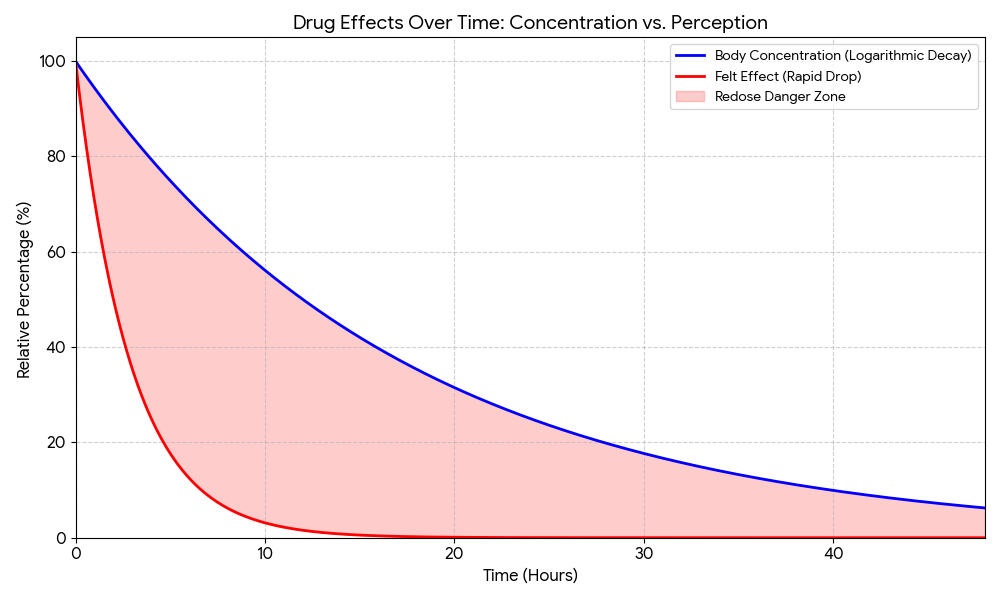
- Active duration - how long the drug is actively having an effect. The "high."
- Half-life - how long it takes the liver to remove 50% of the drug from the entire body. Most hepatic drug metabolism is carried out by CYP450 enzymes (cytochrome P450 - a family of liver enzymes). Individual variation in which CYP450 variants someone carries determines how fast or slow they metabolize a given drug. Two people taking the same dose can have meaningfully different blood concentrations.
The high ends when the drug unbinds and redistributes into fat or blood or when the body adapts in real time.
The drug is still in the body for hours after the felt effect ends.
3.4 LD50 & the Therapeutic Index
Toxicologists measure a substance's killing power with the LD50 - the dose that kills 50% of a test population. It's always written in mg per kg of body weight. Lower number = more toxic.
The ED50 is the effective dose for 50% of the population - the dose that actually does the job. The TI(Therapeutic index) is simply how many multiples of the effective dose you'd need to reach lethality.
Important Note: Tolerance raises the ED50 (you need more for the same effect) but does not consistently raise the LD50 by the same amount.
This course doesn't go deep on LD50 and therapeutic index for specific drugs. Where it's most useful is when you're researching an individual drug on your own: looking up its TI gives you a quick gut-check on how much safety margin exists between a working dose and a dangerous one.
Why LD50 is a rough number and what that means in practice
LD50 figures come mostly from animal studies (rats, mice) and extrapolating to humans involves significant uncertainty. Body size, species metabolism, route of administration, individual variation, and whether the dose is acute or chronic all move the number. Human LD50 data is mostly inferred from overdose case reports rather than controlled trials, for obvious reasons.
In practice the useful takeaway isn't a precise number. It's the ratio. Is this drug's effective dose orders of magnitude below its toxic dose, or are they uncomfortably close? That question matters when you're thinking about drug interactions, tolerance, or route changes (which shift bioavailability and therefore effective plasma concentration).