Empirical Analysis of Addiction Data
The previous modules described mechanisms of addiction at the receptor level. This submodule looks at the population data: of people who use a given drug, how many become addicted? How fast? What predicts the transition?
These numbers come from large epidemiological studies, chiefly the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), the National Survey on Drug Use and Health (NSDUH), and the Epidemiologic Catchment Area study. All have limitations: self-report, recall bias, classification differences across editions of the DSM. Trends across studies are more reliable than any single number.
Lifetime Risk of Dependence Given Any Use
Of people who ever try a substance, the percentage who eventually develop dependence on it (Lopez-Quintero et al., 2011, NESARC; Anthony et al., 1994):
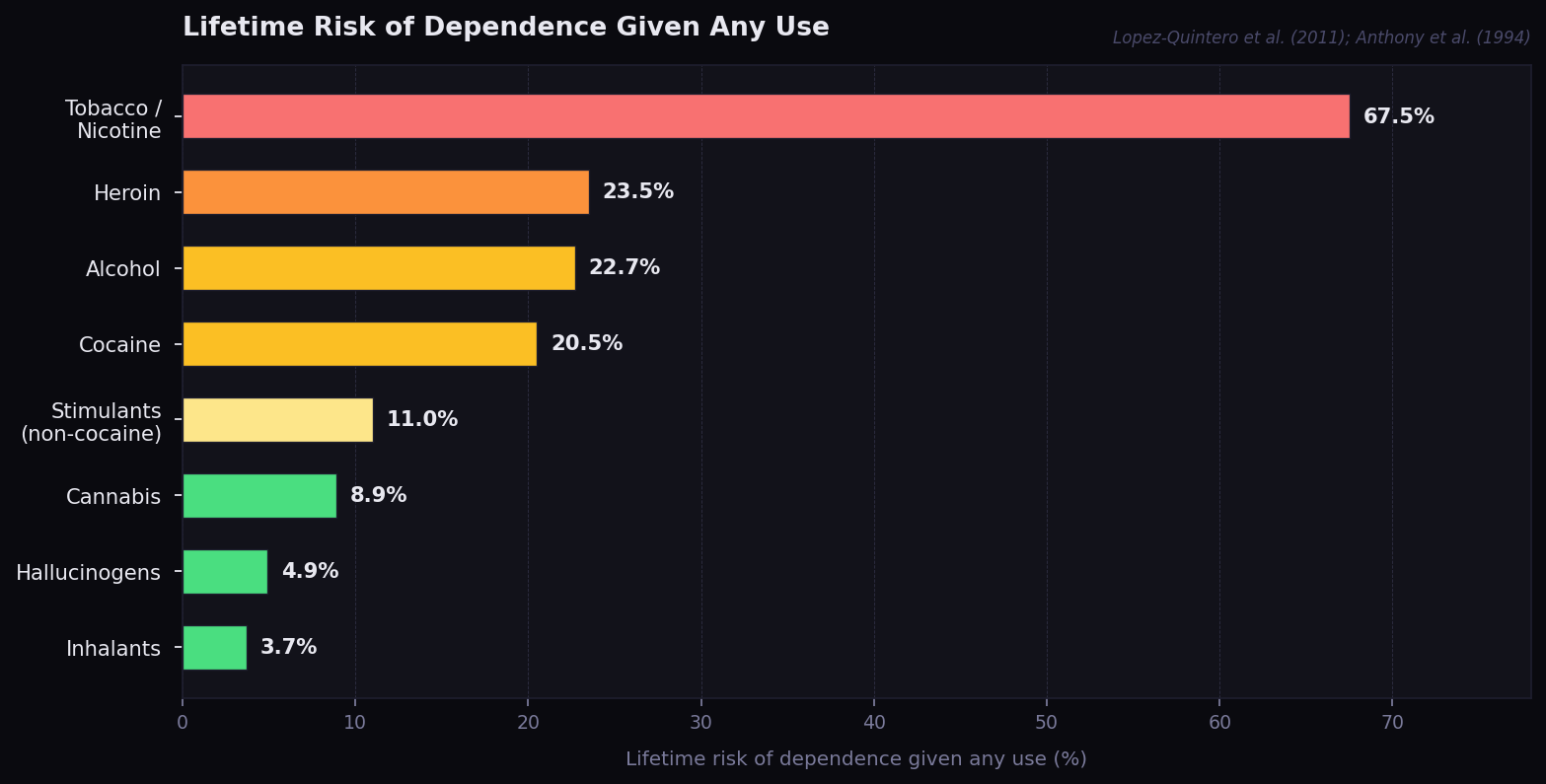
Two patterns stand out:
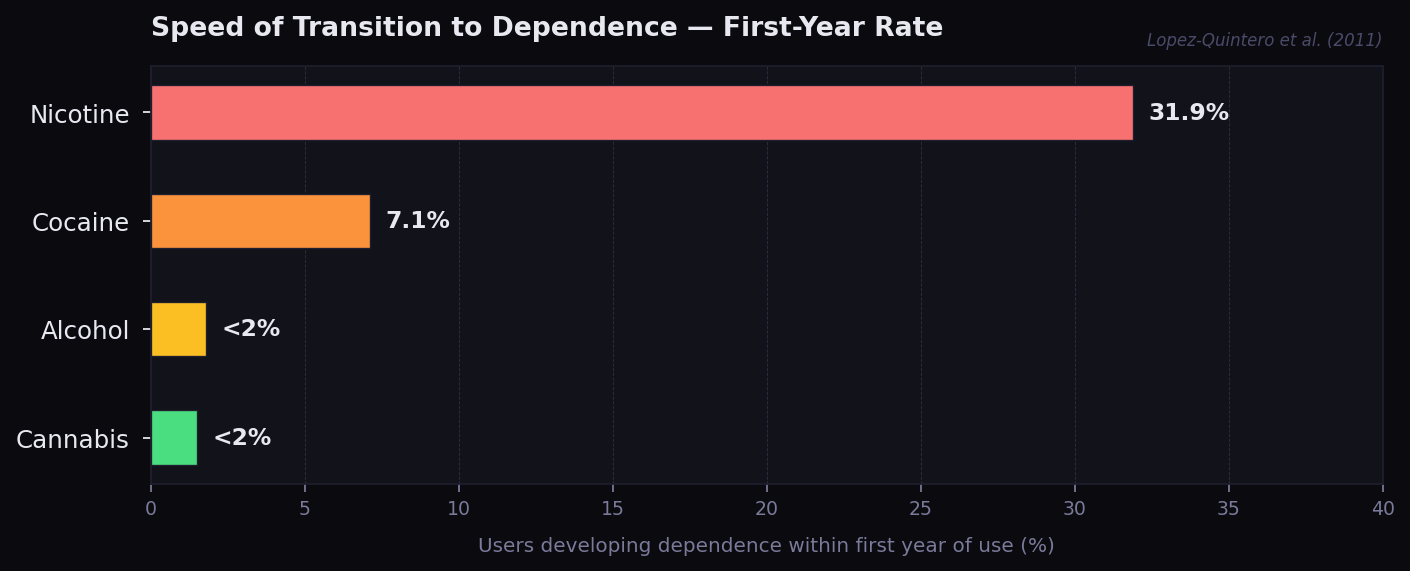
Speed of Transition to Dependence
Among people who become dependent, how fast does it happen after first use? (Lopez-Quintero et al., 2011; Wagner & Anthony, 2002):
- Cocaine: ~7.1% of users develop dependence within the first year of use.
- Cannabis: <2% in first year; median time to dependence ~5–7 years.
- Alcohol: <2% in first year; median time to dependence ~5–10 years.
- Nicotine: highest first-year rates of any drug; many smokers describe dependence within weeks.
- Heroin: rapid; significant first-year transition rates, especially with intravenous use.
Mechanism predicts this. Drugs that produce fast, large dopamine spikes (cocaine, nicotine, IV heroin) trap users faster than drugs that produce slower or smaller signals (alcohol, oral cannabis).
Route of Administration as a Risk Multiplier
Vista Research Group's 2024 follow-up of 10,000 substance-use disorder patients (Vista Research Group, 2025) found one-year abstinence rates differed strongly by route. Note: Vista Research Group is a commercial organization; this report has not been peer-reviewed and should be read alongside the NESARC and NSDUH data above rather than treated equivalently.
- Oral users: highest one-year abstinence rates.
- Injection users: ~34% lower one-year abstinence rates than oral users of the same drug.
Smoking and intravenous routes (both producing fast brain delivery) predict worse long-term outcomes independent of the specific drug.
Genetic Contribution
Twin and adoption studies converge on 40–60% heritability for addiction risk across substances (Volkow & Boyle, 2018; Goldman et al., 2005). This is comparable to the heritability of depression (~40%) and lower than the heritability of schizophrenia (~70%) but higher than the heritability of most personality traits.
Heritability does not mean fate. It means that, of the variation in addiction risk across the population, about half is attributable to genetic differences. The rest is environment, age of first use, mental health comorbidity, social context, and access.
This also does not indicate a purely genetic component, although one could be at play. These patterns could equally reflect environment or trauma being passed down - bad coping mechanisms, learned stress responses, intergenerational patterns of substance use.
Comorbidity
About 60–70% of people with a substance use disorder also have at least one mental health disorder (NSDUH, 2024). The directionality is debated and likely bidirectional: mental health conditions increase drug use risk; chronic drug use increases mental health risk through the receptor-adaptation mechanisms described in earlier modules.
Recovery Statistics
Substance use disorder relapse rates: 40–60% in the year after treatment (NIDA, 2020). Comparable to relapse rates for hypertension or asthma - addiction is a chronic relapsing condition, not a one-shot fix.
One-year abstinence by primary drug (Vista Research Group, 2025, n=10,000; commercial data, non-peer-reviewed):
| Primary drug | 1-year abstinence rate |
|---|---|
| Alcohol | ~41% |
| Amphetamines | ~40% |
| Cannabis | ~38% |
| Methamphetamine | ~31% |
| Fentanyl | ~31% |
| Cocaine | ~30% |
| Heroin | ~29% |
What the Data Says
User Manual
Knowing the population data is not a license to assume "I won't be the unlucky one." Personal risk depends on genetics, mental health, route, frequency, age of first use, and social context, none of which a user can fully evaluate in advance.
If multiple risk factors stack (family history + early first use + smoking/IV route + comorbid mental health condition), the probability of dependence rises substantially above the population baseline.
Conversely, if dependence does develop, the data shows that recovery is achievable. Relapse is part of the process for most people, not a failure.
Sources
- Anthony, J. C., Warner, L. A., & Kessler, R. C. (1994). Comparative epidemiology of dependence on tobacco, alcohol, controlled substances, and inhalants: Basic findings from the National Comorbidity Survey. Experimental and Clinical Psychopharmacology, 2(3), 244–268. https://doi.org/10.1037/1064-1297.2.3.244
- Goldman, D., Oroszi, G., & Ducci, F. (2005). The genetics of addictions: Uncovering the genes. Nature Reviews Genetics, 6(7), 521–532. https://doi.org/10.1038/nrg1635
- Lopez-Quintero, C., et al. (2011). Probability and predictors of transition from first use to dependence on nicotine, alcohol, cannabis, and cocaine: Results of the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Drug and Alcohol Dependence, 115(1–2), 120–130. https://doi.org/10.1016/j.drugalcdep.2010.11.004
- National Institute on Drug Abuse. (2020). Drugs, brains, and behavior: The science of addiction. https://www.drugabuse.gov/publications/drugs-brains-behavior-science-addiction
- Regier, D. A., et al. (1990). Comorbidity of mental disorders with alcohol and other drug abuse: Results from the Epidemiologic Catchment Area (ECA) Study. JAMA, 264(19), 2511–2518. https://doi.org/10.1001/jama.1990.03450190043026
- Substance Abuse and Mental Health Services Administration. (2024). 2023 National Survey on Drug Use and Health (NSDUH). https://www.samhsa.gov/data/release/2023-national-survey-drug-use-and-health-nsduh-releases
- Vista Research Group. (2025). One-year outcomes for 10,000 substance use disorder patients. https://vista-research-group.com/recovery-rates-by-drug
- Volkow, N. D., & Boyle, M. (2018). Neuroscience of addiction: Relevance to prevention and treatment. American Journal of Psychiatry, 175(8), 729–740. https://doi.org/10.1176/appi.ajp.2018.17101174
- Wagner, F. A., & Anthony, J. C. (2002). From first drug use to drug dependence: Developmental periods of risk for dependence upon marijuana, cocaine, and alcohol. Neuropsychopharmacology, 26(4), 479–488. https://doi.org/10.1016/S0893-133X(01)00367-0